
Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia

 ,
,  , , , , , ,
, , , , , , 

Abstract
:1. Introduction
2. Methods
3. Results
3.1. Survey Response
3.2. Demographic Characteristics
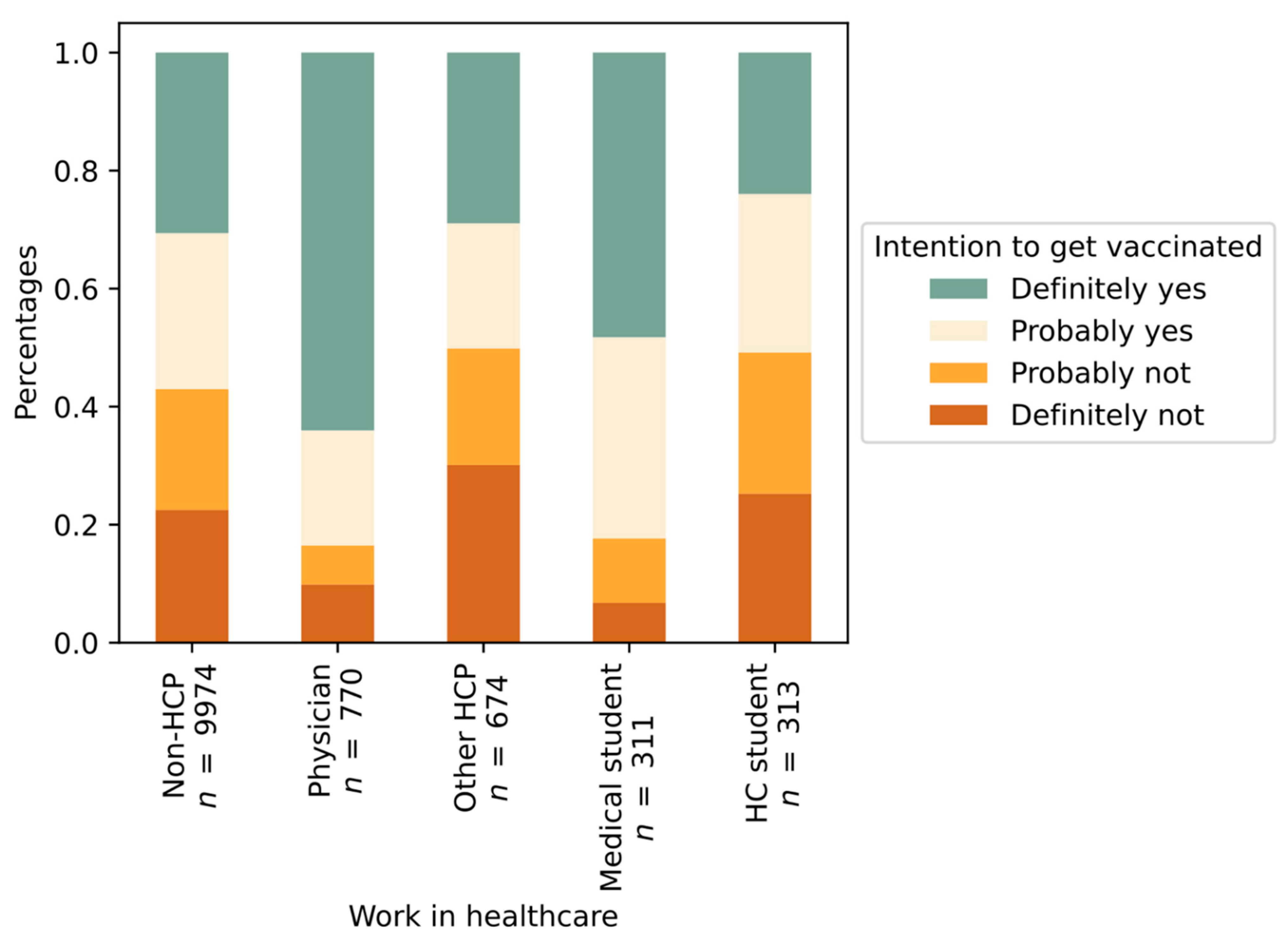
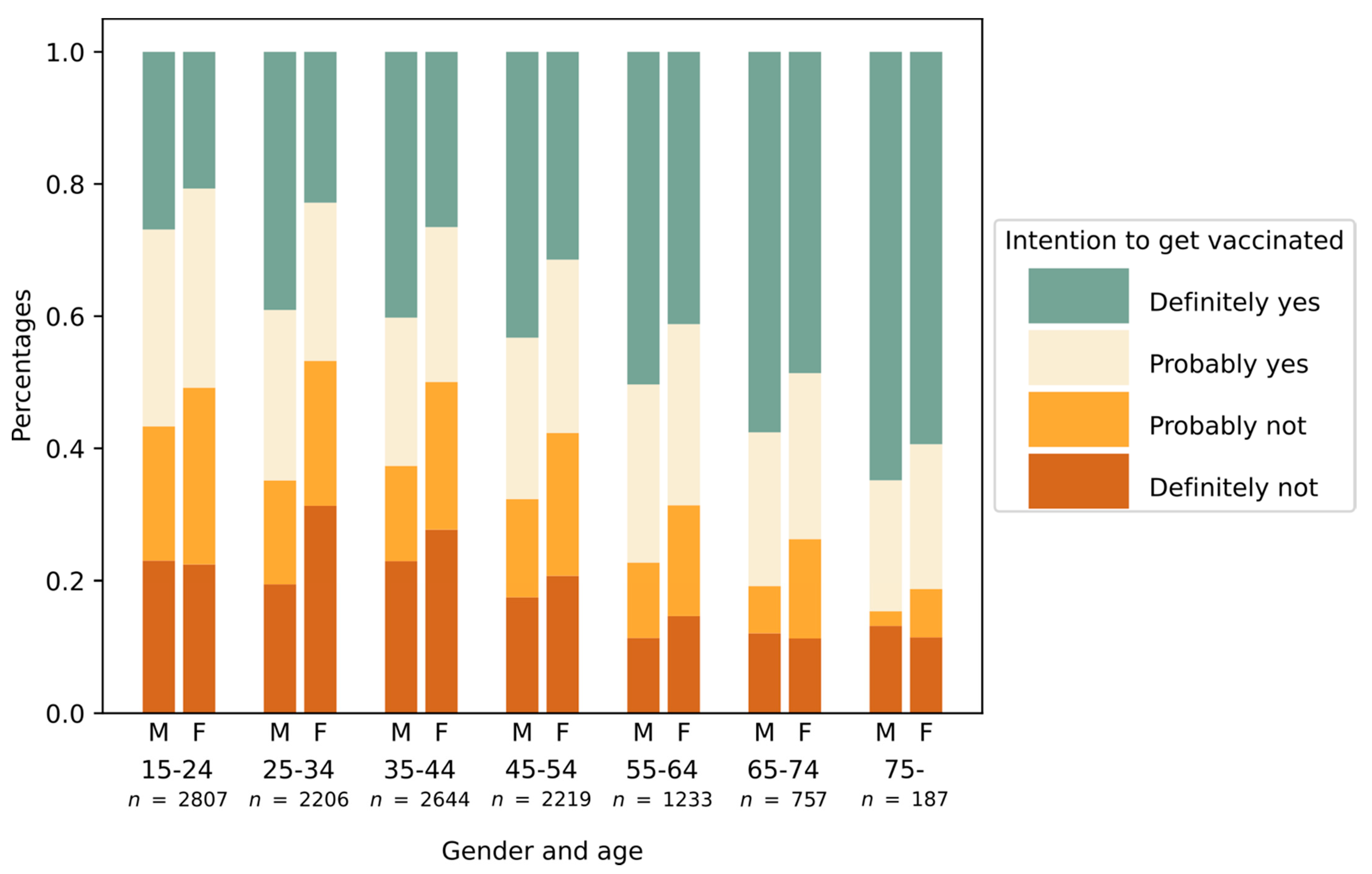
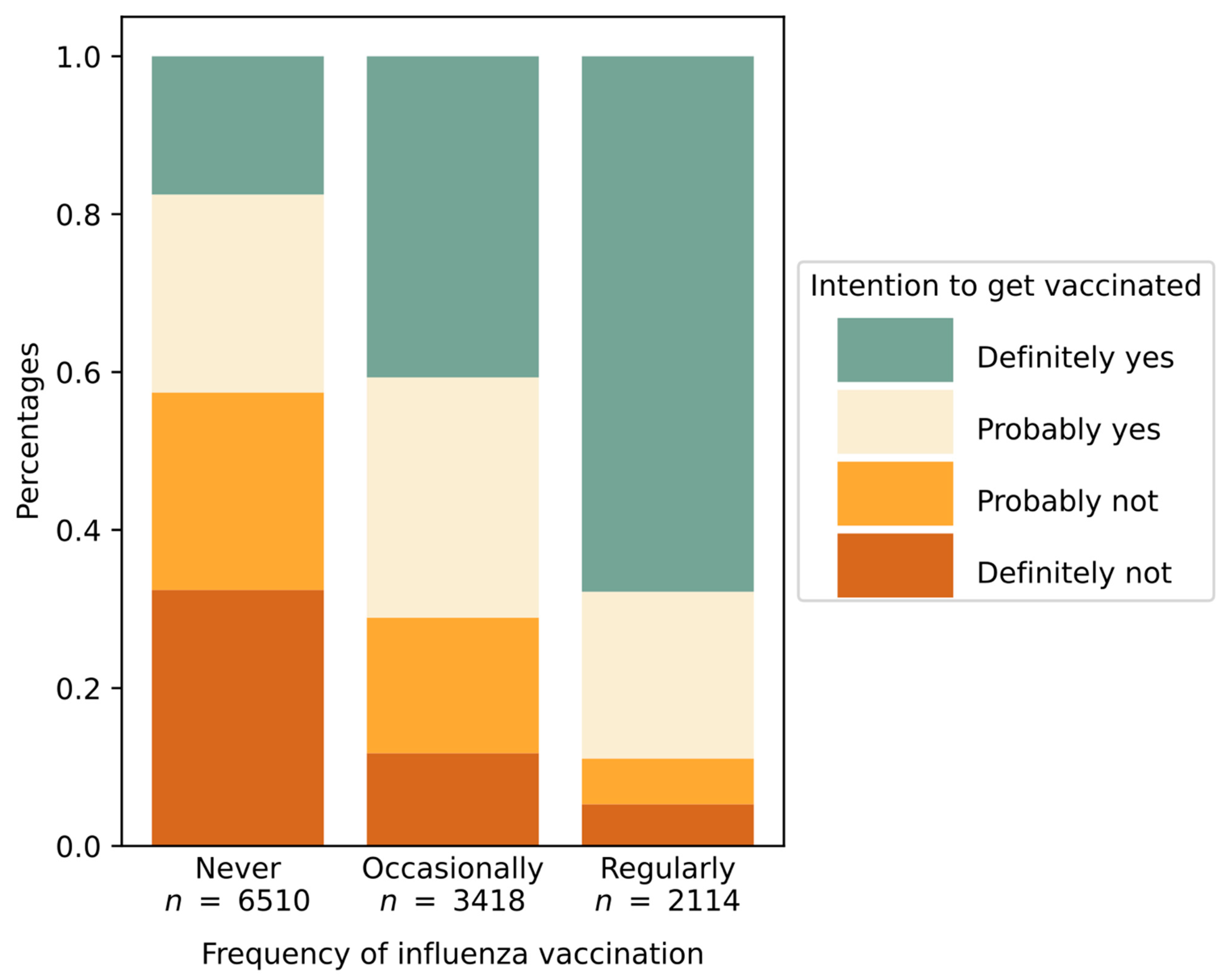
3.3. Intention to Get Vaccinated
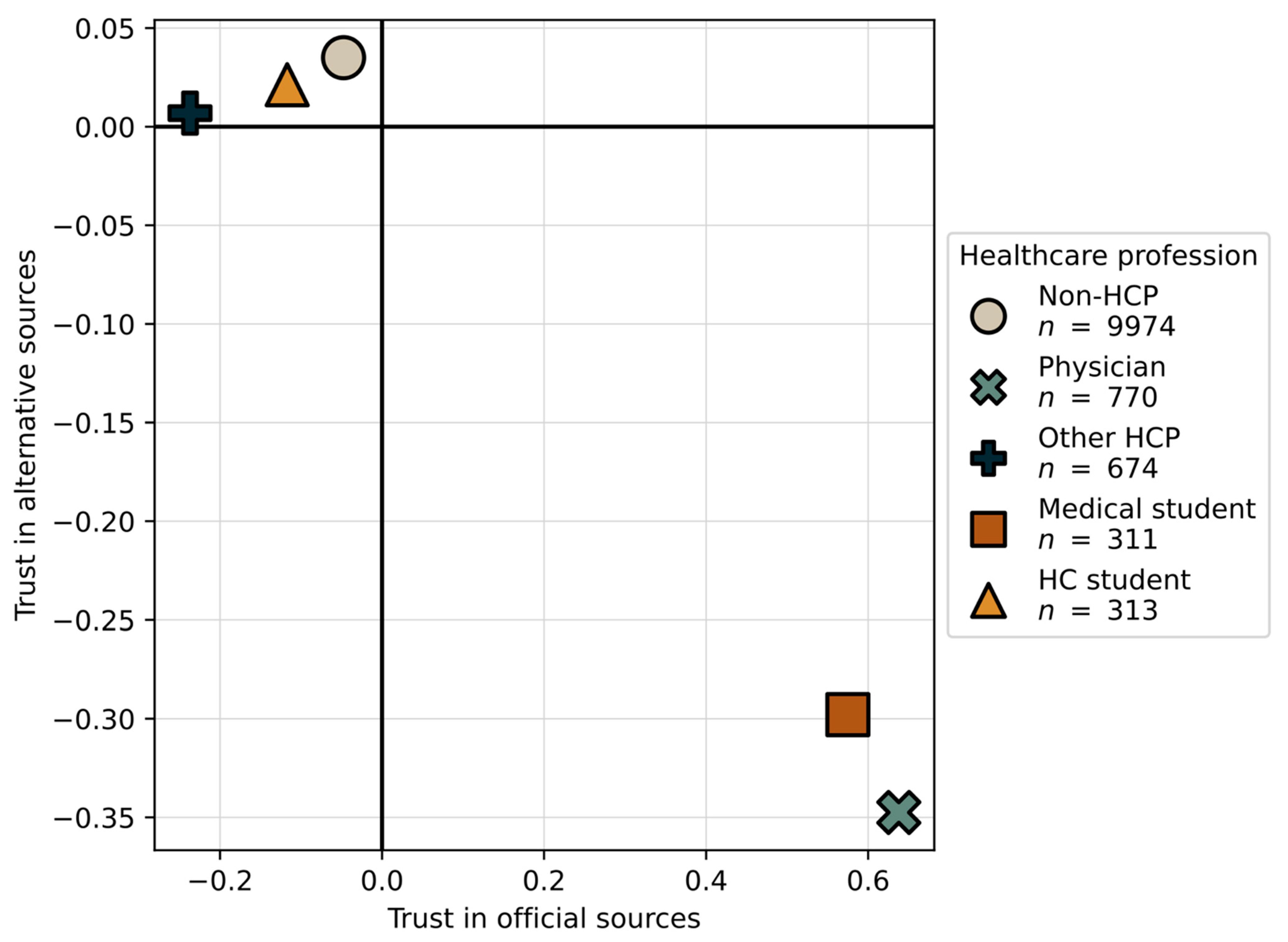
3.4. Principal Component Analysis
3.5. Ordinal Regression
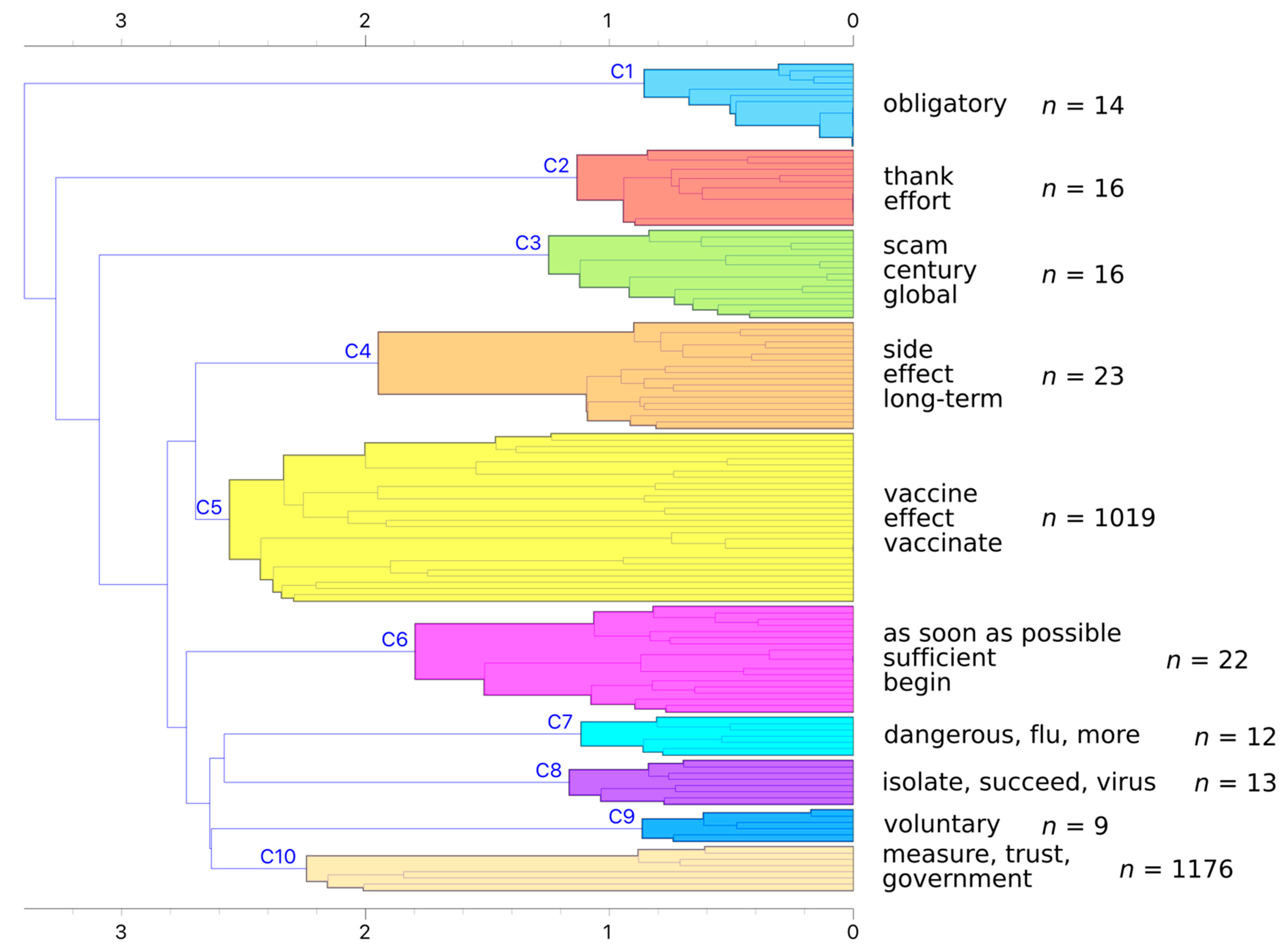
3.6. Analysis of Textual Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Alexandre de, F.; Emilie, K.; Mahesh, R.; Heidi, L. State of Vaccine Confidence in the EU 2018; Health and Food safet Directorate, European Union: Luxembourg, 2018; ISBN 978-92-79-96560-9. [Google Scholar]
- Marcec, R.; Majta, M.; Likic, R. Will vaccination refusal prolong the war on SARS-CoV-2? Postgrad. Med. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kraigher, A.; Voljč, B.; Kamin, T. Cepljenje: Stališča in Odnos Ključnih Javnosti do Cepljenja v Sloveniji; Kraigher, A., Ed.; Nacionalni Inštitut za Javno Zdravje: Ljubljana, Slovenia, 2018; ISBN 978-961-7002-54-6. [Google Scholar]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.J.; Strych, U.; Dor, A.; Franklin Fowler, E.; Motta, M. Correlates and Disparities of COVID-19 Vaccine Hesitancy. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- Straka, M. UDPipe 2.0 prototype at CoNLL 2018 UD shared task. In Proceedings of the CoNLL, Shared Task: Multilingual Parsing from Raw Text to Universal Dependencies, Brussels, Belgium, 31 October–1 November 2018; pp. 197–207. [Google Scholar]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Digital around the world in April 2020—We Are Social. Available online: https://wearesocial.com/blog/2020/04/digital-around-the-world-in-april-2020 (accessed on 7 March 2021).
- Funk, C.; Tyson, A. Intent to Get a COVID-19 Vaccine Rises to 60% as Confidence in Research and Development Process Increases. Pew Research Center. 2020. Available online: www.pewresearch.org. (accessed on 4 January 2021).
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 vaccination during the COVID-19 pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Lindholt, M.F.; Jørgensen, F.J.; Bor, A.; Petersen, M.B. Willingness to Use an Approved COVID-19 Vaccine: Cross-National Evidence on Levels and Individual-Level Predictors. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Graeber, D.; Schmidt-Petri, C.; Schroeder, C. Attitudes on Voluntary and Mandatory Vaccination against COVID-19: Evidence from Germany. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Engin, C.; Vezzoni, C. Who’s Skeptical of Vaccines? Prevalence and Determinants of Anti-Vaccination Attitudes in Italy. Popul. Rev. 2020, 59. [Google Scholar] [CrossRef]
- Ridda, I.; MacIntyre, C.R.; Lindley, R.I. A qualitative study to assess the perceived benefits and barriers to the pneumococcal vaccine in hospitalised older people. Vaccine 2009, 27, 3775–3779. [Google Scholar] [CrossRef] [PubMed]
- Irwin, K.L.; Jalloh, M.B.M.F.; Corker, J.; Alpha Mahmoud, B.; Robinson, S.J.; Li, W.; James, N.E.; Sellu, M.; Jalloh, M.B.M.F.; Diallo, A.A.; et al. Attitudes about vaccines to prevent Ebola virus disease in Guinea at the end of a large Ebola epidemic: Results of a national household survey. Vaccine 2017, 35, 6915–6923. [Google Scholar] [CrossRef] [PubMed]
- Schaffer Deroo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA J. Am. Med. Assoc. 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Head, K.J.; Kasting, M.L.; Sturm, L.A.; Hartsock, J.A.; Zimet, G.D. A National Survey Assessing SARS-CoV-2 Vaccination Intentions: Implications for Future Public Health Communication Efforts. Sci. Commun. 2020, 42, 698–723. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Gadoth, A.; Martin-Blais, R.; Tobin, N.H.; Ferbas, K.G.; Geffen, D.; Aldrovandi, G.M.; Rimoin, A.W. Assessment of COVID-19 vaccine acceptance among healthcare workers in Los Angeles. medRxiv 2020. [Google Scholar] [CrossRef]
- Haviari, S.; Bénet, T.; Saadatian-Elahi, M.; André, P.; Loulergue, P.; Vanhems, P. Vaccination of healthcare workers: A review. Hum. Vaccines Immunother. 2015, 11, 2522–2537. [Google Scholar] [CrossRef] [PubMed]
- Pless, A.; McLennan, S.R.; Nicca, D.; Shaw, D.M.; Elger, B.S. Reasons why nurses decline influenza vaccination: A qualitative study. BMC Nurs. 2017, 16, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwok, K.O.; Li, K.-K.; WEI, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Pers. Individ. Dif. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Dodd, R.H.; Cvejic, E.; Bonner, C.; Pickles, K.; McCaffery, K.J.; Ayre, J.; Batcup, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, 318–319. [Google Scholar] [CrossRef]
- Keske, Ş.; Mutters, N.T.; Tsioutis, C.; Ergönül, Ö. Influenza vaccination among infection control teams: A EUCIC survey prior to COVID-19 pandemic. Vaccine 2020, 38. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Steptoe, A.; Fancourt, D. Anti-Vaccine Attitudes and Risk Factors for Not Agreeing to Vaccination Against COVID-19 Amongst 32,361 UK Adults: Implications for Public Health Communications. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Feleszko, W.; Lewulis, P.; Czarnecki, A.; Waszkiewicz, P. Flattening the Curve of COVID-19 Vaccine Rejection—A Global Overview. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Nuzhath, T.; Tasnim, S.; Sanjwal, R.K.; Trisha, N.F.; Rahman, M.; Mahmud, S.M.F.; Arman, A.; Chakraborty, S.; Hossain, M.M. COVID-19 vaccination hesitancy, misinformation and conspiracy theories on social media: A content analysis of Twitter data. SocArXiv 2020. [Google Scholar] [CrossRef]
- Coustasse, A.; Kimble, C.; Maxik, K. COVID-19 and Vaccine Hesitancy: A Challenge the United States Must Overcome. J. Ambul. Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef]
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; Slavec, A. Attitudes towards SARS-CoV-2 Vaccination—Online Panel Survey [Data File]; University of Ljubljana, Slovenian Social Science Data Archives: Ljubljana, Slovenia, 2020. [Google Scholar] [CrossRef]
- Rus, M.; Groselj, U. Ethics of Vaccination in Childhood-A Framework Based on the Four Principles of Biomedical Ethics. Vaccines 2021, 9, 113. [Google Scholar] [CrossRef]
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; Slavec, A. Attitudes towards SARS-CoV-2 Vaccination—Online Survey [Data File]; University of Ljubljana, Slovenian Social Science Data Archives: Ljubljana, Slovenia, 2020. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Non-HCP | Physicians | Other HCP * | Medical Students | HC Students ** | Total | |
|---|---|---|---|---|---|---|---|
| Gender | Female | 6026 | 537 | 568 | 230 | 266 | 7627 |
| 60.4% | 69.7% | 84.3% | 74.0% | 85.0% | 63.3% | ||
| Male | 3948 | 233 | 106 | 81 | 47 | 4415 | |
| 39.6% | 30.3% | 15.7% | 26.0% | 15.0% | 36.7% | ||
| Age (yr) | 15–24 | 2192 | 7 | 47 | 274 | 287 | 2807 |
| 22.0% | 0.9% | 7.0% | 88.1% | 91.7% | 23.3% | ||
| 25–34 | 1686 | 242 | 223 | 35 | 20 | 2206 | |
| 16.9% | 31.4% | 33.1% | 11.3% | 6.4% | 18.3% | ||
| 35–44 | 2264 | 175 | 192 | 1 | 1 | 2633 | |
| 22.7% | 22.7% | 28.5% | 0.3% | 0.3% | 21.9% | ||
| 45–54 | 1940 | 156 | 119 | 1 | 3 | 2219 | |
| 19.5% | 20.3% | 17.7% | 0.3% | 1.0% | 18.4% | ||
| 55–64 | 1035 | 119 | 79 | 0 | 0 | 1233 | |
| 10.4% | 15.5% | 11.7% | 0.0% | 0.0% | 10.2% | ||
| 65–74 | 679 | 66 | 12 | 0 | 0 | 757 | |
| 6.8% | 8.6% | 1.8% | 0.0% | 0.0% | 6.3% | ||
| ≥75 | 178 | 5 | 2 | 0 | 2 | 187 | |
| 1.8% | 0.6% | 0.3% | 0.0% | 0.6% | 1.6% | ||
| Total | 9974 | 770 | 674 | 311 | 313 | 12,042 | |
| 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | ||
| Principal Component Analysis (PCA): Matrix of Weights | Component | |||
|---|---|---|---|---|
| 1 | 2 | 3 | ||
| Trust in sources of information | Q6a Reports on television and radio. | 0.771 | 0.202 | 0.192 |
| Q6b Daily newspaper. | 0.718 | 0.220 | 0.259 | |
| Q6c National Institute of Public Health. | 0.859 | 0.115 | −0.133 | |
| Q6d The ministry of health of the Republic of Slovenia. | 0.793 | 0.196 | −0.302 | |
| Q6e World Health Organization (WHO). | 0.785 | 0.090 | 0.152 | |
| Q6f The government of the Republic of Slovenia. | 0.556 | 0.186 | −0.626 | |
| Q6g Alternative explanations on social media. | −0.366 | 0.662 | −0.183 | |
| Q6h Professional articles and research findings. | 0.741 | 0.082 | 0.285 | |
| Q6i Expert opinion. | 0.776 | 0.134 | 0.208 | |
| Q6j Information provided to me by acquaintances employed in the field of healthcare. | 0.396 | 0.527 | 0.131 | |
| Q6k Information from friends and acquaintances that are not employed in the field of healthcare. | −0.070 | 0.738 | −0.073 | |
| Agreement with statements | Q10a I trust that the vaccine against SARS-CoV−2 virus is safe. | 0.858 | −0.160 | −0.079 |
| Q10b I believe that vaccination against SARS-CoV-2 virus is effective. | 0.851 | −0.145 | −0.016 | |
| Q10c I would like to wait for more information on the safety of the vaccine against SARS-CoV-2 virus. | −0.214 | 0.292 | 0.473 | |
| Q10d I am very scared of getting infected with SARS-CoV-2 virus. | 0.471 | 0.024 | −0.209 | |
| Q10e I think that SARS-CoV-2 virus is equally dangerous as the influenza virus. | −0.583 | 0.262 | 0.055 | |
| Q10f I have negative experiences with vaccinations—considering me or my loved ones. | −0.608 | 0.255 | −0.078 | |
| Q10g Vaccination against SARS-CoV-2 virus is an attempt of controlling the population. | −0.786 | 0.257 | −0.023 | |
| Intention to Get Vaccinated against COVID-19 | Coef. | Std. Err. | Z | p > |z| | [95% Conf. Interval] | |
|---|---|---|---|---|---|---|
| Age (1 = 15–24, 2 = 25–34,…, 6 = 65–74, 7 = 75+) | 0.487 | 0.028 | 17.170 | 0.000 | 0.431 | 0.542 |
| Gender = male | 0.283 | 0.041 | 6.960 | 0.000 | 0.203 | 0.363 |
| Education = high | −0.200 | 0.043 | −4.680 | 0.000 | −0.283 | −0.116 |
| Experience with COVID-19 (i.e., knew someone who got hospitalised or died from it) | 0.015 | 0.039 | 0.380 | 0.701 | −0.062 | 0.092 |
| Profession = physician | 0.301 | 0.089 | 3.390 | 0.001 | 0.127 | 0.476 |
| Profession = other HCP | 0.123 | 0.084 | 1.460 | 0.144 | −0.042 | 0.289 |
| Profession = medical student | 0.205 | 0.122 | 1.680 | 0.093 | −0.034 | 0.443 |
| Profession = HC student | 0.136 | 0.118 | 1.150 | 0.249 | −0.095 | 0.368 |
| Component 1: Trust in official sources | 2.464 | 0.032 | 77.280 | 0.000 | 2.402 | 2.527 |
| Component 2: Trust in alternative sources | −0.582 | 0.021 | −28.250 | 0000 | −0.622 | −0.541 |
| Component 3: Distrust in government | −0.203 | 0.020 | −10.040 | 0.000 | −0.243 | −0.163 |
| /cut1 | | −1.699 | 0.064 | NA | NA | −1.825 | −1.573 |
| /cut2 | | 0.318 | 0.061 | NA | NA | 0.199 | 0.438 |
| /cut3 | | 2.469 | 0.065 | NA | NA | 2.341 | 2.597 |
| Intention to Get Vaccinated against COVID-19 | % of Total Effect Mediated | [95% Conf. Interval] | Regression Coef. Calculated Based on Direct Effect | |
|---|---|---|---|---|
| Age (1 = 15–24, 2 = 25–34,…, 6 = 65–74, 7 = 75+) | 11.80% | 10.55% | 13.28% | 0.395 |
| Gender = male | 18.19% | 13.88% | 26.00% | 0.231 |
| Education = high | 32.72% | 20.65% | 77.91% | −0.135 |
| Profession = physicians | 100.00% | 82.83% | 355.30% | 0.000 |
| Component 1: Trust in official sources | 5.63% | 5.54% | 5.71% | 2.325 |
| Component 2: Trust in alternative sources | 4.81% | 4.51% | 5.16% | −0.554 |
| Component 3: Distrust in government | 5.13% | 4.26% | 6.49% | −0.193 |
| Subcluster | Description | No. of Answers | |
|---|---|---|---|
| C5.1 | “When will we be able to get the vaccine?” | 91 | |
| C5.1.1 | Vaccine and risk groups | 37 | |
| C5.1.2 | Vaccine availability | 54 | |
| C5.2 | Second thoughts | 928 | |
| C5.2.1 | “I don’t know.” | 7 | |
| C5.2.2 | “We are not test rats.” | 37 | |
| C5.2.3 | Methodological reservations about the survey | 128 | |
| C5.2.4 | “I am worried about side effects.” | 756 | |
| Subcluster | Description | No. of Answers |
|---|---|---|
| C10.1 | “Don’t get vaccinated.” | 7 |
| C10.2 | “Experts should be in higher agreement.” | 172 |
| C10.3 | “We need a vaccine as soon as possible.” | 15 |
| C10.4 | “Vaccine is a genocide.” | 11 |
| C10.5 | Conspiracy theories | 917 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Starešinič, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines 2021, 9, 247. https://doi.org/10.3390/vaccines9030247
Petravić L, Arh R, Gabrovec T, Jazbec L, Rupčić N, Starešinič N, Zorman L, Pretnar A, Srakar A, Zwitter M, et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines. 2021; 9(3):247. https://doi.org/10.3390/vaccines9030247
Chicago/Turabian StylePetravić, Luka, Rok Arh, Tina Gabrovec, Lucija Jazbec, Nika Rupčić, Nina Starešinič, Lea Zorman, Ajda Pretnar, Andrej Srakar, Matjaž Zwitter, and et al. 2021. "Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia" Vaccines 9, no. 3: 247. https://doi.org/10.3390/vaccines9030247