
Treatment, Diagnostic Criteria and Variability of Terminology for Lateral Elbow Pain: Findings from an Overview of Systematic Reviews

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Purpose of the Study
2.3. Search Strategy
2.4. Eligibility Criteria
2.5. Study Selection
2.6. Data Collection
2.7. Quality Assessment
2.8. Agreement
2.9. Data Analysis
3. Results
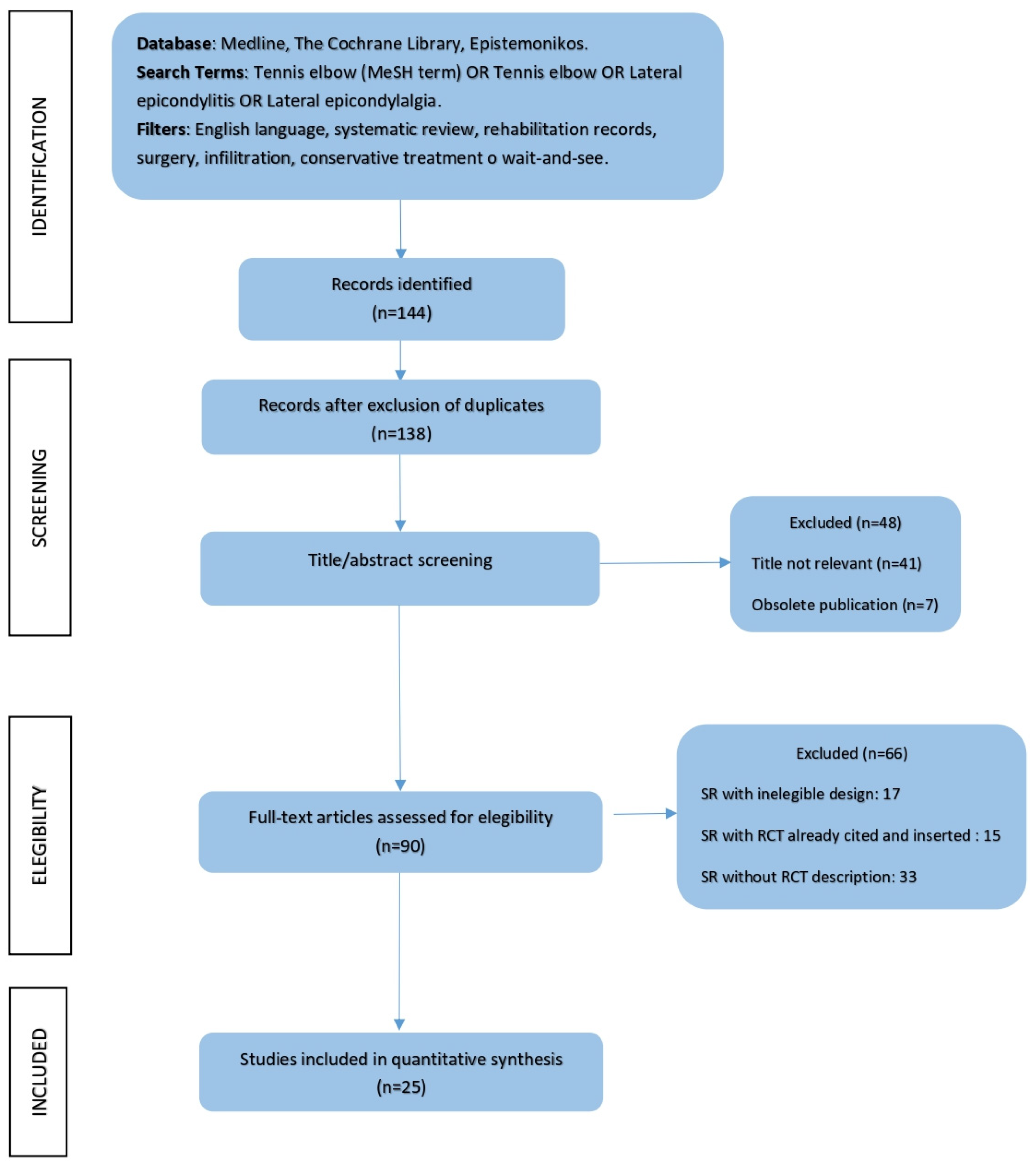
3.1. Study Selection Process
3.2. Characteristics of Treatment and Patients
3.3. Characteristics of the Included Studies
3.4. Risk of Bias of the Included Studies
3.5. Summary of Findings
3.6. Etiopathogenetic Terms in LEP
3.7. Including Criteria in LEP
4. Discussion
4.1. Terminology Variability in LEP
4.2. Classification Based on Onset of Symptoms
4.3. Diagnostic Test in LEP
4.4. Lateral Elbow Disorders: A New Proposal
- (1)
- (2)
- Guiding the clinician in determining whether there is a structure predominantly involved in and responsible for the lateral musculoskeletal disorder of the elbow (muscle–tendon, joint, neural) capable of influencing the prognosis and the type of treatment (conservative and/or surgical); and
- (3)
- Recognising profiles of patients who, depending on the time of suffering, may present the risk of developing yellow flags capable of slowing down or altering the treatment process and/or deteriorating adherence to the therapeutic plan.
- -
- T-LED (Lateral Elbow Disorders—Tendinopathic Prevalence);
- -
- A-LED (Lateral Elbow Disorders—Arthropathic Prevalence);
- -
- N-LED (Lateral Elbow Disorders—Neuropathic Prevalence); and
- -
- M-LED (Lateral Elbow Disorders—Mixed Form).
4.5. Limits
4.6. Consistency
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The following databases were searched • Cochrane Library • Medline | ||
| Search engines used: • PubMed Clinical Queries—Systematic Reviews • Cochrane Review • Epistemonikos | ||
| Pubmed Clinical Queries Search Strategy Tennis elbow [MeSH Term] OR Tennis elbow OR Lateral epicondylitis OR Lateral epicondylalgia OR Lateral elbow tendinopathy | Cochrane Review Search Strategy Tennis elbow OR Lateral epicondylitis OR Lateral epicondylalgia OR Lateral elbow tendinopathy | Epistemonikos Search Strategy Tennis elbow OR Lateral epicondylitis OR Lateral epicondylalgia OR Lateral elbow tendinopathy |
References
- Verhaar, J.A. Tennis elbow. Anatomical, epidemiological and therapeutic aspects. Int. Orthop. 1994, 18, 263–267. [Google Scholar]
- Helliwell, P.S.; Bennett, R.M.; Littlejohn, G.; Muirden, K.D.; Wigley, R.D. Towards epidemiological criteria for soft-tissue disorders of the arm. Occup. Med. 2003, 53, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, P.G. The prevalence of humeral epicondylitis: A survey in general practice. J. R. Coll. Gen. Pract. 1986, 36, 464–465. [Google Scholar] [PubMed]
- Shiri, R.; Viikari-Juntura, E.; Varonen, H.; Heliövaara, M. Prevalence and Determinants of Lateral and Medial Epicondylitis: A Population Study. Am. J. Epidemiol. 2006, 164, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- De Smedt, T.; de Jong, A.; Van Leemput, W.; Lieven, D.; Van Glabbeek, F. Lateral epicondylitis in tennis: Update on aetiology, biomechanics and treatment. Br. J. Sports Med. 2007, 41, 816–819. [Google Scholar] [CrossRef] [PubMed]
- Waugh, E.J.; Jaglal, S.B.; Davis, A.M.; Tomlinson, G.; Verrier, M.C. Factors associated with prognosis of lateral epicondylitis after 8 weeks of physical therapy. Arch. Phys. Med. Rehabil. 2004, 85, 308–318. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. Management of Lateral Elbow Tendinopathy: One Size Does Not Fit All. J. Orthop. Sports Phys. Ther. 2015, 45, 938–949. [Google Scholar] [CrossRef] [Green Version]
- Saroja, G.; Aseer, P.A.L.; Venkata Sai, P.M. Diagnostic accuracy of provocative tests in lateral epicondylitis. Int. J. Physiother. Res. 2014, 2, 815–823. [Google Scholar] [CrossRef]
- Taylor, S.A.; Hannafin, J.A. Evaluation and Management of Elbow Tendinopathy. Sports Health A Multidiscip. Approach 2012, 4, 384–393. [Google Scholar] [CrossRef] [Green Version]
- Herquelot, E.; Bodin, J.; Roquelaure, Y.; Ha, C.; Leclerc, A.; Goldberg, M.; Descatha, A. Work-related risk factors for lateral epicondylitis and other cause of elbow pain in the working population. Am. J. Ind. Med. 2013, 56, 400–409. [Google Scholar] [CrossRef] [Green Version]
- Di Filippo, L.; Pennella, D.; Maselli, F.; Arrigoni, P. Research proposal of a new clinic model for the interpretation of Lateral Elbow Pain: Is it time to change? Muscle Ligaments Tendons J. 2020, 10, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Walz, D.M.; Newman, J.S.; Konin, G.P.; Ross, G. Epicondylitis: Pathogenesis, Imaging, and Treatment. RadioGraphics 2010, 30, 167–184. [Google Scholar] [CrossRef] [Green Version]
- Karanasios, S.; Korakakis, V.; Moutzouri, M.; Drakonaki, E.; Koci, K.; Pantazopoulou, V.; Tsepis, E.; Gioftsos, G. Diagnostic accuracy of examination tests for lateral elbow tendinopathy (LET)—A systematic review. J. Hand Ther. 2021, in press. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Hunt, H.; Pollock, A.; Campbell, P.; Estcourt, L.; Brunton, G. An introduction to overviews of reviews: Planning a relevant research question and objective for an overview. Syst. Rev. 2018, 7, 39. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interven-tions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS Group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Banzi, R.; Cinquini, M.; Gonzalez-Lorenzo, M.; Pecoraro, V.; Capobussi, M.; Minozzi, S. Quality assessment versus risk of bias in systematic reviews: AMSTAR and ROBIS had similar reliability but differed in their construct and applicability. J. Clin. Epidemiol. 2018, 99, 24–32. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research, 1st ed.; Chapman and Hall: London, UK, 1991. [Google Scholar]
- Van der Windt, D.A.; van der Heijden, G.J.; van den Berg, S.G.; Ter Riet, G.; de Winter, A.F.; Bouter, L.M. Ultrasound therapy for musculoskeletal disorders: A systematic review. Pain 1999, 81, 257–271. [Google Scholar] [CrossRef]
- Struijs, P.A.; Smidt, N.; Arola, H.; Van Dijk, C.N.; Buchbinder, R.; Assendelft, W.J. Orthotic devices for tennis elbow: A systematic review. Br. J. Gen. Pr. 2001, 51, 924–929. [Google Scholar]
- Green, S.; Buchbinder, R.; Barnsley, L.; Hall, S.; White, M.; Smidt, N.; Assendelft, W.J. Acupuncture for lateral elbow pain. Cochrane Database Syst. Rev. 2002, 2013, CD003527. [Google Scholar] [CrossRef]
- Borkholder, C.D.; Hill, V.A.; Fess, E.E. The efficacy of splinting for lateral epicondylitis: A systematic review. J. Hand Ther. 2004, 17, 181–199. [Google Scholar] [CrossRef]
- Trudel, D.; Duley, J.; Zastrow, I.; Kerr, E.W.; Davidson, R.; MacDermid, J.C. Rehabilitation for patients with lateral epicondylitis: A systematic review. J. Hand Ther. 2004, 17, 243–266. [Google Scholar] [CrossRef]
- Buchbinder, R.; Green, S.; Youd, J.M.; Assendelft, W.J.; Barnsley, L.; Smidt, N. Shock wave therapy for lateral elbow pain. Cochrane Database Syst. Rev. 2005, 23, 411–414. [Google Scholar] [CrossRef]
- Bisset, L.; Paungmali, A.; Vicenzino, B.; Beller, E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. Br. J. Sports Med. 2005, 39, 411–422. [Google Scholar] [CrossRef] [Green Version]
- Herd, C.R.; Meserve, B.B. A Systematic Review of the Effectiveness of Manipulative Therapy in Treating Lateral Epicondylalgia. J. Man. Manip. Ther. 2008, 16, 225–237. [Google Scholar] [CrossRef]
- Barr, S.; Cerisola, F.L.; Blanchard, V. Effectiveness of corticosteroid injections compared with physiotherapeutic interventions for lateral epicondylitis: A systematic review. Physiotherapy 2009, 95, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: A systematic review of randomised controlled trials. Lancet 2010, 376, 1751–1767. [Google Scholar] [CrossRef] [Green Version]
- Tumilty, S.; Munn, J.; McDonough, S.; Hurley, D.A.; Basford, J.R.; Baxter, G.D. Low Level Laser Treatment of Tendinopathy: A Systematic Review with Meta-analysis. Photomed. Laser Surg. 2010, 28, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Bannuru, R.R.; Severin, M.; Harvey, W. Injection of botulinum toxin for treatment of chronic lateral epi-condylitis: Systematic review and meta-analysis. Semin. Arthritis Rheum. 2011, 40, 532–538. [Google Scholar] [CrossRef]
- Buchbinder, R.; Johnston, R.V.; Barnsley, L.; Assendelft, W.J.; Bell, S.N.; Smidt, N. Surgery for lateral elbow pain. Cochrane Database Syst. Rev. 2011, 2011, CD003525. [Google Scholar] [CrossRef]
- Raman, J.; MacDermid, J.C.; Grewal, R. Effectiveness of Different Methods of Resistance Exercises in Lateral Epicondylosis—A Systematic Review. J. Hand Ther. 2012, 25, 5–26. [Google Scholar] [CrossRef]
- Ahmad, Z.; Brooks, R.; Kang, S.-N.; Weaver, H.; Nunney, I.; Tytherleigh-Strong, G.; Rushton, N. The Effect of Platelet-Rich Plasma on Clinical Outcomes in Lateral Epicondylitis. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Pattanittum, P.; Turner, T.; Green, S.; Buchbinder, R. Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database Syst. Rev. 2013, 2013, CD003686. [Google Scholar] [CrossRef]
- Cullinane, F.L.; Boocock, M.G.; Trevelyan, F.C. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clin. Rehabil. 2014, 28, 3–19. [Google Scholar] [CrossRef]
- Tang, H.; Fan, H.; Chen, J.; Yang, M.; Yi, X.; Dai, G.; Chen, J.; Tang, L.; Rong, H.; Wu, J.; et al. Acupuncture for Lateral Epicondylitis: A Systematic Review. Evidence-Based Complement. Altern. Med. 2015, 2015, 861849. [Google Scholar] [CrossRef] [Green Version]
- Tsikopoulos, K.; Tsikopoulos, A.; Natsis, K. Autologous whole blood or corticosteroid injections for the treatment of epi-condylopathy and plantar fasciopathy? A systematic review and meta-analysis of randomized controlled trials. Phys. Ther. Sport 2016, 22, 114–122. [Google Scholar] [CrossRef]
- Mattie, R.; Wong, J.; McCormick, Z.; Yu, S.; Saltychev, M.; Laimi, K. Percutaneous Needle Tenotomy for the Treatment of Lateral Epicondylitis: A Systematic Review of the Literature. PM R 2017, 9, 603–611. [Google Scholar] [CrossRef]
- Burn, M.B.; Mitchell, R.J.; Liberman, S.R.; Lintner, D.M.; Harris, J.D.; McCulloch, P.C. Open, Arthroscopic, and Percutaneous Surgical Treatment of Lateral Epicondylitis: A Systematic Review. Hand 2017, 13, 264–274. [Google Scholar] [CrossRef]
- Lucado, A.M.; Dale, R.B.; Vincent, J.; Day, J.M. Do joint mobilizations assist in the recovery of lateral elbow tendinopathy? A systematic review and meta-analysis. J. Hand Ther. 2018, 32, 262–276. [Google Scholar] [CrossRef]
- Lin, Y.-C.; Wu, W.-T.; Hsu, Y.-C.; Han, D.-S.; Chang, K.-V. Comparative effectiveness of botulinum toxin versus non-surgical treatments for treating lateral epicondylitis: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Santana, M.J.; Sanchez-Infante, J.; Gómez-Chiguano, G.F.; Cleland, J.A.; López-De-Uralde-Villanueva, I.; Fernández-De-Las-Peñas, C.; Manzano, G.P. Effects of trigger point dry needling on lateral epicondylalgia of musculoskeletal origin: A systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1327–1340. [Google Scholar] [CrossRef] [PubMed]
- Karanasios, S.; Korakakis, V.; Whiteley, R.; Vasilogeorgis, I.; Woodbridge, S.; Gioftsos, G. Exercise interventions in lateral elbow tendinopathy have better outcomes than passive interventions, but the effects are small: A systematic review and meta-analysis of 2123 subjects in 30 trials. Br. J. Sports Med. 2020, 55, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Major, H.P. Lawn-tennis Elbow. BMJ 1883, 2, 557. [Google Scholar]
- Khan, K.M.; Cook, J.L.; Kannus, P.; Maffulli, N.; Bonar, S.F. Time to abandon the ‘tendinitis’ myth. BMJ 2002, 324, 626–627. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, J.T.; Baptista, J.S.; Vaz, M. Incidence and prevalence of upper-limb work related musculoskeletal disorders: A systematic review. Work 2015, 51, 635–644. [Google Scholar] [CrossRef]
- Maffulli, N.; Testa, V.; Capasso, G.; Ewen, S.W.; Sullo, A.; Benazzo, F.; King, J.B. Similar Histopathological Picture in Males with Achilles and Patellar Tendinopathy. Med. Sci. Sports Exerc. 2004, 36, 1470–1475. [Google Scholar] [CrossRef]
- Cook, J.L.; Purdam, C.R. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br. J. Sports Med. 2009, 43, 409–416. [Google Scholar] [CrossRef] [Green Version]
- Rio, E.; Kidgell, D.; Moseley, L.; Gaida, J.; Docking, S.; Purdam, C.; Cook, J. Tendon neuroplastic training: Changing the way we think about tendon rehabilitation: A narrative review. Br. J. Sports Med. 2015, 50, 209–215. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. A new integrative model of lateral epicondylalgia. Br. J. Sports Med. 2009, 43, 252–258. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Carnero, J.; Fernandez-de-Las-Penas, C.; de la Llave-Rincon, A.I.; Ge, H.-Y.; Arendt-Nielsen, L. Widespread mechanical pain hypersensitivity as sign of central sensitization in unilateral epicondylalgia: A blinded, controlled study. Clin. J. Pain 2009, 25, 555–561. [Google Scholar] [CrossRef]
- Kim, J.K.; Park, M.G.; Shin, S.J. What is the Minimum Clinically Important Difference in Grip Strength? Clin. Orthop. Relat. Res. 2014, 472, 2536–2541. [Google Scholar] [CrossRef] [Green Version]
- Lim, E.C.W. Pain Free Grip Strength test. J. Physiother. 2013, 59, 59. [Google Scholar] [CrossRef]
- Vicenzino, B.; Paungmali, A.; Buratowski, S.; Wright, A. Specific manipulative therapy treatment for chronic lateral epicon-dylalgia produces uniquely characteristic hypoalgesia. Man Ther. 2001, 6, 205–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drechsler, W.; Knarr, J.F.; Snyder-Mackler, L. A Comparison of Two Treatment Regimens for Lateral Epicondylitis: A Randomized Trial of Clinical Interventions. J. Sport Rehabil. 1997, 6, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Moradi, A.; Ebrahimzadeh, M.H.; Jupiter, J.B. Radial Tunnel Syndrome, Diagnostic and Treatment Dilemma. Arch. Bone Jt. Surg. 2015, 3, 156–162. [Google Scholar]
- Arrigoni, P.; Cucchi, D.; D’Ambrosi, R.; Butt, U.; Safran, M.R.; Denard, P.; Randelli, P. Intra-articular findings in symptomatic minor instability of the lateral elbow (SMILE). Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2255–2263. [Google Scholar] [CrossRef]
- Kniesel, B.; Huth, J.; Bauer, G.; Mauch, F. Systematic diagnosis and therapy of lateral elbow pain with emphasis on elbow instability. Arch. Orthop. Trauma. Surg. 2014, 134, 1641–1647. [Google Scholar] [CrossRef]
- Vlaeyen, J.; Morley, S.; Linton, S.; Boersma, K.; De Jong, J. Pain-Related Fear: Exposure-Based Treatment for Chronic Pain; IASP Press: Washington, DC, USA, 2012. [Google Scholar]
- Pennella, D.; Giagio, S.; Maselli, F.; Fiorentino, F.; Brindisino, F. Red flags useful to screen for gastrointestinal and hepatic diseases in patients with shoulder pain: A scoping review. Musculoskelet. Care 2022. [Google Scholar]
- Maselli, F.; Palladino, M.; Barbari, V.; Storari, L.; Rossettini, G.; Testa, M. The diagnostic value of Red Flags in thoracolumbar pain: A systematic review. Disabil. Rehabil. 2020, 44, 1190–1206. [Google Scholar] [CrossRef] [PubMed]
- Maselli, F.; Testa, M. Superficial peroneal nerve schwannoma presenting as lumbar radicular syndrome in a non-competitive runner. J. Back Musculoskelet. Rehabil. 2019, 32, 361–365. [Google Scholar] [CrossRef]
- Mourad, F.; Maselli, F.; Patuzzo, A.; Siracusa, A.; Di Filippo, L.; Dunning, J.; de Las Peñas, C.F. Osteocohondritis dissecans of the radial head in a young athlete: A case report. Int. J. Sports Phys. Ther. 2018, 13, 726–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bialosky, J.E.; Bishop, M.D.; Price, D.D.; Robinson, M.E.; George, S.Z. The mechanisms of manual therapy in the treatment of musculoskeletal pain: A comprehensive model. Man. Ther. 2009, 14, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Zusman, M. The Modernisation of Manipulative Therapy. Int. J. Clin. Med. 2011, 2, 644–649. [Google Scholar] [CrossRef] [Green Version]
- Bishop, M.D.; Torres-Cueco, R.; Gay, C.W.; Lluch-Girbes, E.; Beneciuk, J.M.; Bialosky, J.E. What effect can manual therapy have on a patient’s pain experience? Pain Manag. 2015, 5, 455–464. [Google Scholar] [CrossRef] [Green Version]
- Rio, E.; Moseley, L.; Purdam, C.; Samiric, T.; Kidgell, D.; Pearce, A.J.; Jaberzadeh, S.; Cook, J. The pain of tendinopathy: Physiological or pathophysiological? Sports Med. 2014, 44, 9–23. [Google Scholar] [CrossRef]
- Arrigoni, P.; Cucchi, D.; Menon, A.; Randelli, P. It’s time to change perspective! New diagnostic tools for lateral elbow pain. Musculoskelet. Surg. 2017, 101, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Hing, W.; Hall, T.; Rivett, D.; Vicenzino, B.; Mulligan, B. The Mulligan Concept of Manual Therapy, 1st ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Bula-Oyola, E.; Belda-Lois, J.-M.; Porcar-Seder, R.; Page, A. Effectiveness of electrophysical modalities in the rehabilitation of radial, ulnar, and median neuropathies. PLoS ONE 2021, 16, e0248484. [Google Scholar] [CrossRef]
- Boyer, M.I.; Hastings, H., II. Lateral tennis elbow: Is there any science out there? J. Shoulder Elbow Surg. 1999, 8, 481–491. [Google Scholar] [CrossRef]
- Nimgade, A.; Sullivan, M.; Goldman, R. Physiotherapy, Steroid Injections, or Rest for Lateral Epicondylosis? What the Evidence Suggests. Pain Pr. 2005, 5, 203–215. [Google Scholar] [CrossRef]
- Nirschl, R.P.; Ashman, E.S. Elbow tendinopathy: Tennis elbow. Clin. Sports Med. 2003, 22, 813–836. [Google Scholar] [CrossRef]




| Review Year Country | Review Aim | Search Strategy | Studies and Participants | Patients, Interventions, Comparison, Outcome, and Study Type (PICOS) | Risk of Bias | Limits | Author’s Conclusion |
|---|---|---|---|---|---|---|---|
| van der Windt et al. (1999) [21] The Netherlands | To evaluate the effectiveness of ultrasound therapy in the treatment of musculoskeletal disorders and lateral epicondylitis (LE). | MEDLINE, EMBASE No search start date. Last search date in July 1997. Search terms defined. No limitation described. RCTs were screened. No evidence of reference checking. Eligibility criteria: patients with pain and/or restriction of range of motion associated with musculoskeletal disorders, RCTs, English. | RCT s= 4 N = 123 | Population: patients with lateral epicondylitis Intervention: US Comparison: US sham, low-level laser, exercise Study type: RCTs | No evidence of quality assessment | Only RCTs in the US and LE were included. | The findings reported for lateral epicondylitis were less consistent and may warrant further evaluation. |
| Struijs et al. (2002) [22] Australia | To determine the efficacy of treatment of lateral epicondylitis by an orthotic device. | MEDLINE, EMBASE, CINAHL. No search start date. Last search date in 1999. Search terms defined. No limitations described. RCTs were screened. No evidence of reference checking. Eligibility criteria: patients with lateral epicondylitis of the humerus (tennis elbow), RCTs, English. | RCTs = 5 N = 300 | Population: patients with lateral epicondylitis Intervention: orthotic devices Comparison: corticosteroid injection, anti-inflammatory cream, splintage, physiotherapy Study type: RCTs | Clear quality appraisal of the studies | A standard set of valid and reliable outcome measures should be incorporated into the RCTs. | No definitive conclusions can be drawn concerning the effectiveness of orthotic devices for lateral epicondylitis. More well-designed and well-conducted RCTs of sufficient power are warranted. |
| Green et al. (2002) [23] Australia | To determine the effectiveness of acupuncture in the treatment of patients with lateral elbow pain with respect to symptom reduction, including pain, improvement in function, grip strength, and adverse effects. | MEDLINE, EMBASE, CINAHL No search start date. Last search date in June 2001. Search terms defined. No limitations described. RCTs were screened. Evidence of reference checking. Eligibility criteria: lateral elbow pain and acupuncture, RCTs, English. | RCTs = 4 N = 239 | Population: patients with lateral epicondylitis Intervention: acupuncture Comparison: sham acupuncture, low-level laser, vitamin B12 Study type: RCTs | Quality assessment completed but criteria and explanation unclear. | Trials should be adequately powered, attempt to blind both participants, including outcome measures of pain and function and adverse effects. | There is insufficient evidence to either support or refute the use of acupuncture (either needle or laser) in the treatment of lateral elbow pain. |
| Borkholder et al. (2004) [24] USA | To confirm or refute the efficacy of using splints in the treatment of lateral epicondylitis. | CINAHL, EMBASE, PEDro, and Cochrane databases. No search start date. Last search date in December 2003. Search terms defined. No limitations described. RCTs were screened. Evidence of hand searching. Eligibility criteria: splint and lateral elbow pain, RCTs, English. | RCTs = 8 N = 347 | Population: patients with lateral epicondylitis Intervention: splinting Comparison: other splint, manipulation, anti-inflammatory cream, diclofenac Study type: RCTs | Clear quality appraisal of the studies. | Duration of symptoms was not considered in the majority of the included studies. | Early positive, but not conclusive, support for the effectiveness of splinting lateral epicondylitis. |
| Trudel et al. (2004) [25] Canada | To determine the effectiveness of conservative treatments for lateral epicondylitis and to provide recommendations based on this evidence. | CINAHL, EMBASE, PEDro, and Cochrane databases. Search start date 1983. Last search date in March 2003. Search terms defined. No limitations described. RCTs were screened. Evidence of hand searching. Eligibility criteria: English, adults (age 18+), humans, RCTs or quasi-RCTs, lateral epicondylitis, and rehabilitation. | RCTs = 21 N = 1666 | Population: patients with lateral epicondylitis Intervention: US, acupuncture, rebox, wait-and-see, exercise, mobilisation, ionisation, laser, pulsed electromagnetic field Comparison: phonophoresis, sham, injection Study type: RCTs | Clear quality appraisal of the studies. | No adequate blinding measures, follow-up, and standardised outcome measures in RCTs. | There is a number of good-quality studies on various therapeutic interventions for lateral epicondylitis that demonstrate a variety of effective treatment options. |
| Buchbinder et al. (2004) [26] Australia | To determine the effectiveness and safety of shockwaves (ESWT) in the treatment of adults with lateral elbow pain. | MEDLINE, CINAHL, EMBASE, SCISEARCH, Cochrane Clinical Trials trial database. No search start and finish date. Search terms defined. No limitations described. RCTs were screened. No eligibility criteria. | RCT = 2 N = 372 | Population: patients with lateral epicondylitis Intervention: ESWT Comparison: placebo ESWT Study type: RCTs | Quality assessment completed but criteria and explanation unclear. | Unclear allocation procedures in the trial of Rompe et al. and the treatment allocation of those who dropped out of the trial (13% of participants) was not reported. | The effectiveness of ESWT is unclear. The two trials included in this review yielded conflicting results. Further trials are needed to clarify the value of ESWT for lateral elbow pain. |
| Bisset et al. (2005) [27] Australia | To look at the effectiveness of physical interventions on clinically relevant outcomes for LE. | MEDLINE, CINAHL, EMBASE, Web of Science, Allied and Complimentary Medicine, SPORTDiscus, PEDro. Last search date in September 2003. Search terms defined. No limitations described. RCTs were screened. Eligibility criteria: RCT, English, patient with lateral elbow pain. | RCTs = 24 N = 1760 | Population: patients with lateral epicondylitis Intervention: laser, ESWT, manipulation, mobilisation, exercise tape, orthotics, acupuncture, laser, iontophoresis Comparison: sham ESWT, sham tape, sham acupuncture Study type: RCTs | Clear quality appraisal of the studies. | Duration of symptoms and follow-up was not considered in the majority of included studies. | Evidence is accruing that does not support the use of ESWT, but there is indication for further research with long-term follow-up into manipulation and exercise as forms of treatment for LE. |
| Herd, (2008) [28] The Netherlands | To review the effectiveness of manipulation in treating lateral epicondylalgia. | MEDLINE, Cumulative Index of Nursing and Allied Health Literature, Health Source, SPORTDiscus, Physiotherapy Evidence Database. Search start date 1929. Last search date in November 2007. Search terms defined. No limitations described. RCTs were screened. No evidence of reference checking. Eligibility criteria: English, experimental design, subjects with lateral epicondylitis, manipulative treatment. | RCTs = 13 N = 639 | Population: patients with lateral epicondylitis Intervention: manipulative therapy, Cyriax, MWM Comparison: exercise, injection, wait-and-see, US, friction massage Study type: RCTs | Clear quality appraisal of the studies. | Variability regarding manipulative technique, comparison interventions, follow-up, and outcome measures. Only one reviewer determined appropriateness for inclusion. | Current evidence supports Mulligan’s mobilisation with movement not only in providing immediate benefits but also improving outcomes at short- and long-term follow-up. A subgroup of patients with LE exists who would benefit from treatment directed at the cervical spine. |
| Barr et al. (2009) [29] UK | To compare the effectiveness of corticosteroid injections with physiotherapeutic interventions for the treatment of lateral epicondylitis (tennis elbow). | AMED, MEDLINE, CINAHL, EMBASE, Cochrane Central Register of Controlled Clinical Trials, Metaregister of Controlled Clinical Trials, PEDro. Search start date 1966. Last search date in March 2009. Search terms defined. No limitations described. RCTs were screened. Evidence of hand searching. Eligibility criteria: English, RCTs, lateral epicondylitis and corticosteroid injection. | RCTs = 3 N = 596 | Population: patients with lateral epicondylitis Intervention: corticosteroid injection, corticosteroid injection with exercise and manipulation Comparison: exercise, US, wait-and-see, paracetamol, no treatment Study type: RCTs | Clear quality appraisal of the studies. | No follow-up in RCTs, no similar outcome measures. | Corticosteroid injections are effective at short-term follow-up, and physiotherapeutic interventions are effective at intermediate- and long-term follow-up. However, any conclusions drawn must be interpreted with caution. |
| Coombes et al. (2010) [30] Australia | To review the clinical efficacy and risk of adverse events of injections (including corticosteroids) for treatment of tendinopathy in the short term, intermediate term, and long term, and in different areas of tendinopathy. | MEDLINE, CINAHL, EMBASE, Web of Knowledge, Allied and Complementary Medicine, SPORTDiscus, Cochrane Controlled Trial Register, and Physiotherapy Evidence Database. No starting data search. Last search date in March 2010. Search terms defined. No limitations described. RCTs were screened. Evidence of hand searching. Eligibility criteria: RCTs, tendinopathy, and injection. | RCTs = 12 N = 1034 | Population: patients with tendinopathy Intervention: corticosteroid injection, corticosteroid injection with exercise Comparison: physiotherapy, wait-and-see, NSAIDs, manipulation. Study type: RCTs | Clear quality appraisal of the studies. | No concealed allocation and similar outcome measures in the majority of included RCTs. | Despite the effectiveness of corticosteroid injections in the short term, non-corticosteroid injections might be of benefit for long-term treatment of lateral epicondylalgia. However, response to injection should not be generalised because of variation in effect between sites of tendinopathy. |
| Tumilty et al. (2010) [31] New Zealand | To assess the clinical effectiveness of low-level laser therapy (LLLT) in the treatment of tendinopathy. | MEDLINE, PubMed, CINAHL, AMED, EMBASE, All EBM (Evidence-Based Medicine) reviews, PEDro (Physiotherapy Evidence Database), SCOPUS. No starting data search. Last search date in August 2008. Search terms defined. No limitations described. RCTs were screened. No evidence of reference checking. Eligibility criteria: RCT, tendinopathy, and LLLT. | RCTs = 12 (10) N = 422 | Population: patients with tendinopathy Intervention: LLLT Comparison: placebo, Tecar, friction massage, corticosteroid injection Study type: RCTs | Clear quality appraisal of the studies. | Only RCTs on LLLT and LE were included. Poor blinding procedures and reliable outcome measures. | LLLT can potentially be effective in treating tendinopathy when recommended dosages are used. The 12 positive studies provide strong evidence that positive outcomes are associated with the use of current dosage recommendations for the treatment of tendinopathy. |
| Kalichman et al. (2011) [32] Israel | To determine the efficacy of botulinum toxin for the treatment of chronic lateral epicondylitis. | PubMed, MEDLINE, CINAHL, Google Scholar, EMBASE, PEDro, ISI web of Science databases. No starting data search. Last search date in November 2009. Search terms defined. No limitations described. RCTs were screened. Evidence of hand searching. Eligibility criteria: botulinum toxin A for treatment of lateral epicondylitis, RCTs. | RCTs = 4 N = 278 | Population: patients with lateral epicondylitis Intervention: botulinum toxin A injection Comparison: placebo (saline solution) Study type: RCTs | Clear quality appraisal of the studies. | No concealed allocation, description of adverse effect, and similar outcome measures in the majority of included RCTs. | Current literature provides support for use of botulinum toxin A injections into the forearm extensor muscles (60 units Disport or equivalent) for the treatment of chronic treatment-resistant lateral epicondylitis. |
| Buchbinder at al. (2011) [33] Australia | To determine the benefits and safety of surgery for lateral elbow pain. | CENTRAL (The Cochrane Library), MEDLINE, EMBASE, CINAHL, and Web of Science. Search start date 1966. Last search date in December 2010. Search terms defined. No limitations described. RCTs were screened. No evidence of hand searching. Eligibility criteria: lateral elbow pain and surgery. | RCTs = 5 N = 193 | Population: patients with lateral epicondylitis Intervention: “open” surgery, percutaneous surgery Comparison: percutaneous surgery, botulinum toxin, ESWT Study type: RCTs | Clear quality appraisal of the studies. | Trials were susceptible to bias and hampered by inadequate reporting and small sample size. | Due to a small number of studies, large heterogeneity in interventions across trials, small sample sizes, and poor reporting of outcomes, there is insufficient evidence to support or refute the effectiveness of surgery for lateral elbow pain. |
| Raman et al. (2012) [34] Canada | To synthesise the quality and content of clinical research addressing type and dosage of resistance exercises in lateral epicondylosis | MEDLINE, EMBASE, CINAHL, SCOPUS. Search start date 1966. Last search date in December 2010. Search terms defined. Studies that investigated surgery, orthoses (splints), shock wave therapy, electrical stimulation, steroid injections, or casts were excluded. RCTs were screened. No evidence of hand searching. Eligibility criteria: lateral epicondylosis and exercise (strength, resistance, eccentric, concentric) | RCTs = 9 N = 697 | Population: patients with lateral epicondylitis Intervention: resistance training (isometric, eccentric, concentric, isokinetic) Comparison: static stretching, ice, manipulation, forearm band; US Study type: RCTs | Clear quality appraisal of the studies. | Lack of high-quality trials that compared different exercise types or dosage, and a lack of detailed descriptions of exercise parameters in many published studies. | Strengthening using resistance exercises is effective in reducing pain and improving function for lateral epicondylosis, but optimal dosing is not defined. |
| Ahmad et al. (2013) [35] UK | To evaluate the evidence for the application of platelet-rich plasma (PRP) in lateral epicondylitis. | MEDLINE, EMBASE, CINAHL PubMed. Search start date 1966. Last search date in 2011. Search terms defined. No limitations described. RCTs were screened. No evidence of hand searching. Eligibility criteria: Human, RCTs, English, PRP in patients with lateral epicondylitis. | RCTs = 8 N = 507 | Population: patients with lateral epicondylitis Intervention: PRP Comparison: saline injection, placebo Study type: RCTs | Clear quality appraisal of the studies. | Heterogeneity of patient population, variation of PRP preparation, and lack of standard outcome measures. | Limited but evolving evidence for the use of PRP in lateral epicondylitis; however, further research is required to understand the concentration and preparation that facilitate the best clinical outcome. |
| Pattanittum et al. (2013) [36] Australia | To assess the benefits and harm of topical and oral NSAIDs for treating people with lateral elbow pain. | MEDLINE, EMBASE, CINAHL, Cochrane. Search start date 1966. Last search date in 2011. Search terms defined. No limitations described. RCTs were screened. No evidence of hand searching. Eligibility criteria: Human, RCTs, NSAIDs in lateral elbow pain. | RCTs = 14 N = 938 | Population: patients with lateral epicondylitis Intervention: NSAIDs Comparison: placebo Study type: RCTs | Clear quality appraisal of the studies. | RCTs did not provide enough published data, or did not provide data in a form that could be extracted for meta-analysis. | Limited evidence from which to draw firm conclusions about the benefits or harm of topical or oral NSAIDs in treating lateral elbow pain. |
| Cullinane et al. (2014) [37] New Zealand | To establish the effectiveness of eccentric exercise as a treatment intervention for lateral epicondylitis. | ProQuest, Medline via EBSCO, AMED, Scopus, Web of Science, CINAHL No starting search date. Last search date in 2011. Search terms defined. Limits: corticosteroid injections prior to the intervention or as part of the treatment or comparative therapy. RCTs were screened. No evidence of hand searching. Eligibility criteria: English, RCTs, tennis elbow, and eccentric exercise. | RCTs = 12 (3) N = 611 | Population: patients with lateral epicondylitis Intervention: Eccentric exercise, eccentric exercise with other therapies Comparison: iontophoresis, US, stretching Study type: RCTs | Quality assessment completed but criteria and explanation unclear. | Lack of blinding of participants and treatment providers, lack of control group and standardised diagnostic criteria. | The majority of consistent findings support the inclusion of eccentric exercise as part of a multimodal therapy programme for improved outcomes in patients with lateral epicondylitis. |
| Tang et al. (2015) [38] China | To assess the effectiveness and safety of acupuncture for lateral epicondylitis (LE). | EMBASE, PubMed, the Cochrane Library, China National Knowledge Infrastructure (CNKI), Chinese Scientific Journal Database (VIP database), Wanfang Database, and Chinese Biomedical Literature Database (Sinomed). No starting search date. Last search date in 2015. Search terms defined. Limitations: no laser stimulation, no acupressure, no other type of acupuncture. RCTs were screened. No evidence of reference and hand searching. Eligibility criteria: RCTs, acupuncture, and lateral epicondylitis. | RCTs = 4 N = 309 | Population: patients with lateral epicondylitis Intervention: acupuncture, electro-acupuncture Comparison: sham acupuncture, blockage therapy Study type: RCTs | Quality assessment completed but criteria and explanation unclear. | No detailed definition on random sequence generation, allocation concealment, and blinding of participants and personnel. | For the small number of included studies with poor methodological quality, no firm conclusion can be drawn regarding the effect of acupuncture on elbow functional status and myodynamia for LE. |
| Tsikopoulos et al. (2016) [39] Greece | To compare the efficacy of autologous whole blood with that of corticosteroid injections on epicondylopathy and plantar fasciopathy (PF). | PubMed, Web of Science, CENTRAL, and Scopus. No starting search date. Last search date on 6 May 2015. Search terms defined. No limitations described. Evidence of reference and hand searching. Eligibility criteria: Human, English, RCTs, autologous venous blood with that of corticosteroids on either epicondylopathy or PF. | RCTs = 9 (5) N = 447 (209) | Population: patients with lateral epicondylitis Intervention: autologous whole-blood intervention, corticosteroid injection Comparison: autologous whole-blood intervention, corticosteroid injection, placebo Study type: RCTs | Clear quality appraisal of the studies. | Eight RCTs were conducted in Asia. The follow-up in eight studies did not exceed six months. | Corticosteroids were marginally superior to autologous whole blood in relieving pain on plantar fasciopathy at 2–6 weeks. Autologous whole blood provided significant clinical relief on epicondylopathy at 8–24 weeks. Conclusions were limited by the risk of bias. |
| Mattie et al. (2017) [40] USA | To analyse currently available controlled studies on percutaneous tenotomy and its efficacy for the treatment of lateral epicondylitis. | MEDLINE, EMBASE, CINAHL, Cochrane, Web of Science. No starting search date. Last search date in November 2015. Search terms defined. No limitations described. Evidence of reference and hand searching. Eligibility criteria: English, RCTs, tennis elbow, and percutaneous tenotomy. | RCTs = 6 N = 242 | Population: patients with lateral epicondylitis Intervention: percutaneous tenotomy Comparison: / Study type: prospective studies | Quality assessment completed but criteria and explanation unclear. | The included RCTs had a small sample size and patient self-selection for The procedure. The studies included variability of time in follow-up and in duration of symptoms. | Percutaneous tenotomy presents an alternative to surgical release of the common extensor tendon for the treatment of chronic tendinosis at the lateral epicondyle of the elbow. Current research supporting the efficacy of this procedure, however, is of low quality (level II to level IV). |
| Burn et al. (2017) [41] USA | To determine whether the choice of surgical technique (open, percutaneous, or arthroscopic) would lead to significantly different clinical outcomes in lateral epicondylitis (LE). | PubMed, Cochrane Central Register of Controlled Trials, and Google Scholar. No starting search date. Last search date in July 2016. Search terms defined. No limitations described. Evidence of reference and hand searching. Eligibility criteria: English, RCTs, tennis elbow, and surgery treatment. | RCTs = 5 N = 179 | Population: patients with lateral epicondylitis Intervention: open, percutaneous or arthroscopic intervention Comparison: open, percutaneous or arthroscopic intervention Study type: RCTs | Quality assessment completed but criteria and explanation unclear. | Performance bias is present as the surgical interventions and postoperative protocols were not identical for all studies. There was a wide heterogeneity in surgical procedures and outcome measures used in the included studies. | There are no clinically significant differences between the 3 surgical techniques (open, arthroscopic, and percutaneous) in terms of functional outcome (DASH), pain intensity (VAS), and patient satisfaction at 1-year follow-up in subjects with LE. |
| Lucado et al. (2018) [42] USA | To determine whether joint mobilisations are effective in improving pain, grip strength, and disability in adults with LET. | CINAHL, PubMed, and PEDro. No starting search date. Last search date in June 2017. Search terms defined. No limitations described. Evidence of reference and hand searching. Eligibility criteria: RCTs, English, mobilisation or manipulation, and lateral elbow tendinopathy. | RCTs = 6 (3) N = 461 (205) | Population: patients with lateral epicondylitis Intervention: MWM, manipulation, mobilisation Comparison: US, corticosteroid, placebo injection, traditional treatment Study type: RCTs | Clear quality appraisal of the studies. | There were very few studies with similar research design, outcomes, or follow-up time periods. | There is compelling evidence that joint mobilisations have a positive effect on both pain and/or functional grip scores across all time frames compared to control groups in the management of LET. |
| Lin et al. (2018) [43] Taiwan | To explore the effectiveness of botulinum toxin compared with non-surgical treatments in patients with lateral epicondylitis. | PubMed, Scopus, Embase, and Airity Library. No starting search date. Last search date in February 2017. Search terms defined. No limitations described. Evidence of reference and hand searching. Eligibility criteria: RCTs, English and Chinese, lateral epicondylitis, and botulinum toxin. | RCTs = 6 N = 310 | Population: patients with lateral epicondylitis Intervention: botulinum toxin injection Comparison: placebo injection Study type: RCTs | Clear quality appraisal of the studies. | Not all the RCTs documented other possible adverse events, including infection, tingling sensation, and tenderness related to injections. | When treating lateral epicondylitis, botulinum toxin was superior to placebo and could last for 16 weeks. Corticosteroid and botulinum toxin injections were largely equivalent, except the corticosteroid injections were better at pain relief in the early stages and were associated with less weakness in grip in the first 12 weeks. |
| Navarro-Santana et al. (2020) [44] Spain | To evaluate the effect of dry needling alone or combined with other treatment interventions on pain, related-disability, pressure pain sensitivity, and strength in people with lateral epicondylalgia of musculoskeletal origin. | MEDLINE, CINAHL, PubMed, PEDro, Cochrane Library, SCOPUS, and Web of Science databases from their inception to 5 April 2020. | RCTs = 7 N = 320 | Population: patients with lateral epicondylitis Intervention: trigger-point dry needling Comparison: low-level laser, manipulation, ultrasound, ESWT Study type: RCTs | Clear quality appraisal of the studies. | The number of included trials was small (n = 7). Additionally, needling interventions were applied with different dosages. Another potential limitation is the heterogeneity and imprecision of the results of some of the trials. | The current meta-analysis found low evidence supporting the application of dry needling for the treatment of lateral epicondylalgia of musculoskeletal origin; however, some questions remain to be elucidated in future studies. |
| Karanasios et al. (2021) [45] Greece | To evaluate the effectiveness of exercise compared with other conservative interventions in the management of LET. | MEDLINE, PubMed, CINAHL, EMBASE, PEDro, ScienceDirect, Cochrane Library, and Grey literature databases were systematically searched from inception to November 2019. | RCTs = 30 N = 2123 | Population: patients with lateral epicondylitis Intervention: exercise Comparison: exercise, manipulation, corticosteroid, wait-and-see Study type: RCTs | Clear quality appraisal of the studies. | Despite including 30 studies with over 2000 participants, there were no studies with a low risk of bias. | Low and very low certainty evidence suggests exercise is effective compared with passive interventions with or without invasive treatment in LET, but the effect is small. |
| Review Year Country | TERMINOLOGY ADOPTED | TREATMENT |
|---|---|---|
| van der Windt et al. (1999) [21] The Netherlands | Tennis elbow, lateral epicondylitis, lateral epicondylalgia, epicondylalgia | Ultrasound (US) |
| Struijs et al. (2002) [22] Australia | Tennis elbow, lateral epicondylitis | Orthotic devices |
| Green et al. (2002) [23] Australia | Tennis elbow, epicondylalgia | Acupuncture |
| Borkholder et al. (2004) [24] USA | Tennis elbow, lateral epicondylitis | Splinting |
| Trudel et al. (2004) [25] Canada | Tennis elbow, epicondylalgia | US, acupuncture, rebox, wait-and-see, exercise, mobilisation, ionisation, laser, pulsed electromagnetic field |
| Buchbinder et al. (2004) [26] Australia | Tennis elbow | ESWT |
| Bisset et al. (2005) [27] Australia | Tennis elbow, lateral epicondylitis, extensor carpi radial tendinitis, epicondylalgia | Laser, ESWT, manipulation, mobilisation, exercise tape, orthotics, acupuncture, iontophoresis |
| Herd (2008) [28] The Netherlands | Tennis elbow, lateral epicondylitis, lateral epicondylalgia | Manipulative therapy, Cyriax, mobilisation with movement (MWM) |
| Barr et al. (2009) [29] UK | Lateral epicondylitis | Corticosteroid injection, corticosteroid injection with exercise, manipulation |
| Coombes et al. (2010) [30] Australia | Tennis elbow, lateral epicondylitis, lateral epicondylalgia, epicondylalgia, lateral elbow pain | Corticosteroid injection, corticosteroid injection with exercise |
| Tumilty et al. (2010) [31] New Zealand | Tennis elbow, lateral epicondylitis, extensor carpi radial tendinitis, epicondylalgia | LLLT |
| Kalichman et al. (2011) [32] Israel | Tennis elbow, lateral epicondylitis | Botulinum toxin A injection |
| Buchbinderat al. (2011) [33] Australia | Tennis elbow, lateral epicondylitis | “Open” surgery, percutaneous surgery |
| Raman et al. (2012) [34] Canada | Tennis elbow, lateral epicondylitis, lateral elbow tendinopathy, epicondylosis, lateral epicondylar tendinopathy | Resistance training (isometric, eccentric, concentric, isokinetic) |
| Ahmad et al. (2013) [35] UK | Lateral epicondylitis, lateral elbow tendinopathy, chronic elbow tendinosis | PRP |
| Pattanittumet al. (2013) [36] Australia | Tennis elbow, lateral epicondylitis | NSAIDs |
| Cullinane et al. (2014) [37] New Zealand | Tennis elbow, lateral epicondylalgia | Eccentric exercise, eccentric exercise with other therapies |
| Tang et al. (2015) [38] China | Tennis elbow, lateral epicondylitis | Acupuncture, electro-acupuncture |
| Tsikopouloset al. (2016) [39] Greece | Tennis elbow, lateral epicondylitis, lateral elbow tendinopathy | Autologous whole-blood intervention, corticosteroid injection |
| Mattie et al. (2017) [40] USA | Tennis elbow, lateral epicondylitis, common extensor tendinosis | Percutaneous tenotomy |
| Burn et al. (2017) [41] USA | Tennis elbow, lateral epicondylitis | Open, percutaneous, or arthroscopic intervention |
| Lucado et al. (2018) [42] USA | Lateral epicondylitis, lateral epicondylalgia | MWM, manipulation, mobilisation |
| Lin et al. (2018) [43] Taiwan | Tennis elbow, lateral epicondylitis | Botulinum toxin injection |
| Navarro-Santana et al. (2020) [44] Spain | Tennis elbow, lateral epicondylitis, lateral elbow tendinopathy | Trigger-point dry needling |
| Karanasios et al. (2021) [45] Greece | Tennis elbow, lateral epicondylitis, lateral elbow tendinopathy, epicondylalgia | Eccentric exercise, isometric exercise, corticosteroid, manipulation |
| Review Year Country | PHASE 2 | PHASE 3 | |||
| 1. Study Eligibility Criteria | 2. Identification and Selection of Studies | 3. Data Collection and Study Appraisal | 4. Synthesis and Findings | Risk of Bias in the Review | |
| van der Windt et al. (1999) [21] The Netherlands |  | | |  | |
| Struijs et al. (2002) [22] Australia | | | | | |
| Green et al. (2002) [23] Australia | | | | | |
| Borkholder et al. (2004) [24] USA | | | | | |
| Trudel et al. (2004) [25] Canada | | | | | |
| Buchbinder et al. (2004) [26] Australia | | |  | | |
| Bisset et al. (2005) [27] Australia | | | | | |
| Herd (2008) [28] The Netherlands | | | | | |
| Barr et al. (2009) [29] UK | | | | | |
| Coombes et al. (2010) [30] Australia | | | | | |
| Tumilty et al. (2010) [31] New Zealand | | | | | |
| Kalichman et al. (2011) [32] Israel | | | | | |
| Buchbinder at al. (2011) [33] Australia | | | | | |
| Raman et al. (2012) [34] Canada | | | | | |
| Ahmad et al. (2013) [35] UK | | | | | |
| Pattanittum et al. (2013) [36] Australia | | | | | |
| Cullinane et al. (2014) [37] New Zealand | | | | | |
| Tang et al. (2015) [38] China | | | | | |
| Tsikopoulos et al. (2016) [39] Greece | | | | | |
| Mattie et al. (2017) [40] USA | | | | | |
| Burn et al. (2017) [41] USA | | | | | |
| Lucado et al. (2018) [42] USA | | | | | |
| Lin et al. (2018) [43] Taiwan | | | | | |
| Navarro-Santana et al. (2020) [44] Spain | | | | | |
| Karanasios et al. (2021) [45] Greece | | | | | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Filippo, L.; Vincenzi, S.; Pennella, D.; Maselli, F. Treatment, Diagnostic Criteria and Variability of Terminology for Lateral Elbow Pain: Findings from an Overview of Systematic Reviews. Healthcare 2022, 10, 1095. https://doi.org/10.3390/healthcare10061095
Di Filippo L, Vincenzi S, Pennella D, Maselli F. Treatment, Diagnostic Criteria and Variability of Terminology for Lateral Elbow Pain: Findings from an Overview of Systematic Reviews. Healthcare. 2022; 10(6):1095. https://doi.org/10.3390/healthcare10061095
Chicago/Turabian StyleDi Filippo, Luigi, Simone Vincenzi, Denis Pennella, and Filippo Maselli. 2022. "Treatment, Diagnostic Criteria and Variability of Terminology for Lateral Elbow Pain: Findings from an Overview of Systematic Reviews" Healthcare 10, no. 6: 1095. https://doi.org/10.3390/healthcare10061095