
Abstract
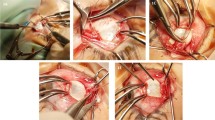
Background Measurement of recession in strabismus surgery is performed either from the limbus or from the muscle insertion. These measurement methods may result in inaccuracies that may influence the outcome of the procedure. We prospectively evaluated the outcome of recessions measured from the extraocular muscle suture site to its insertion in an incidence cohort.
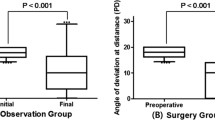
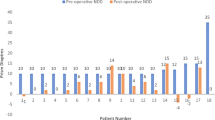
Methods Thirty-six consecutive surgical procedures for infantile esotropia and 23 for constant exotropia were performed in which measurements were performed from the suture site. A successful surgery for esotropia was defined as an orthophoria of up to +10 prism dioptres of deviation for non- accommodative targets at a distance of 20 feet, measured by cover and prism test. A successful surgery for exotropia was defined as a residual deviation between −10 and +10 prism dioptres. The statistical significance of the outcome influencing factors was assessed by chi-square test.
Results Six weeks following surgery, 28 procedures (78%) for infantile and non- accommodative esotropia and 19 procedures (83%) for exotropia were successful. At the end of the follow-up period (mean 13.7 months ± 9.4 for esotropia and 11.6 months 12.8 for exotropia), the success rate was 77% for esotropia and 75% for exotropia. Prematurity and mental retardation in esotropia, exotropia with pre-operative deviations larger than −45 prism dioptres and amblyopia in exotropia were related to unfavourable outcome (p < 0.05).
Conclusions Measurement for muscle recession can be performed from the suture site. The outcome is comparable to the outcome when measurements are performed from the limbus or the insertion, probably due to the incidence cohort. Refinement of the technique and defining other factors influencing the outcome of strabismus surgery may improve the outcome.
Similar content being viewed by others
Article PDF
References
Helveston EM, Ellis FD, Patterson JH, Weber J . Augmented recession of the medial recti. Ophthalmology 1987;85:507–11.
Helveston EM, Ellis FD, Schott J, Mitchelson J, Weber JC, Taube S, Miller K . Surgical treatment of congenital esotropia. Am J Ophthalmol 1983;96:218–28.
Kushner BJ, Morton GV . A randomized comparison of surgical procedures for infantile esotropia. Am J Ophthalmol 1984;98:50–61.
Hess JB, Calhoun JH . A new rationale for the management of large angle esotropia. J Pediatr Ophthalmol Strabismus 1979;16:345–8.
Fisher NF, Flom NC, Jampolsky A . Early surgery of congenital esotropia. Am J Ophthalmol 1968;65:439–43.
Prieto-Diaz J . Large bilateral medial rectus recession in early esotropia with bilateral limitation of abduction. J Pediatr Ophthalmol Strabismus 1980;17:101–5.
Nelson LB, Calhoun JH, Simon JW, Wilson T, Harley RD . Surgical management of large angle congenital esotropia. Br J Ophthalmol 1987;71:380–3.
Kushner BJ, Luckhese NJ, Morton GV . Should recession of the medial recti be graded from the limbus or insertion? Arch Ophthalmol 1989;107:1755-8.
Nelson LB, Wagner RS, Simon JW, Harley RD . Congenital esotropia. Surv Ophthalmol 1987;31:363–83.
Kushner BJ, Preslan MW, Vrabec M . Artifacts of measuring during strabismus surgery. J Pediatr Ophthalmol Strabismus 1987;24:159–64.
Keenan JM, Willshaw HE . Outcome of strabismus surgery in congenital esotropia. Br J Ophthalmol 1992;76:342–5.
Keenan JM, Willshaw HE . The outcome of strabismus surgery in childhood esotropia. Eye 1993;7:341–5.
Keenan JM, Willshaw HE . The outcome of strabmismus surgery in childhood exotropia. Eye 1994;8:632–7.
Gillies WE, McIndol A . Measurement of strabismus eyes with A-scan ultrasonography. Aust J Ophthalmol 1981;9:321–2.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Segal, Z., Rehany, U. & Rumelt, S. Measurements for horizontal extraocular muscle surgery from the suture site: Outcome and influencing factors. Eye 14, 879–883 (2000). https://doi.org/10.1038/eye.2000.241
Received:
Revised:
Issue Date:
DOI: https://doi.org/10.1038/eye.2000.241
