
Abstract
Ambulance data has been reported to be a sensitive indicator of health service use during hot days, but there is no comprehensive summary of the quantitative association between heat and ambulance dispatches. We conducted a systematic review and meta-analysis to retrieve and synthesise evidence published up to 31 August 2022 about the association between heat, prolonged heat (i.e. heatwaves), and the risk of ambulance dispatches. We initially identified 3628 peer-reviewed papers and included 48 papers which satisfied the inclusion criteria. The meta-analyses showed that, for each 5 °C increase in mean temperature, the risk of ambulance dispatches for all causes and for cardiovascular diseases increased by 7% (95% confidence interval (CI): 5%, 10%) and 2% (95% CI: 1%, 3%), respectively, but not for respiratory diseases. The risk of ambulance dispatches increased by 6% (95% CI: 4%, 7%), 7% (95% CI: 5%, 9%), and 18% (95% CI: 12%, 23%) under low-intensity, severe, and extreme heatwaves, respectively. We observed two potential sources of bias in the existing literature: (1) bias in temperature exposure measurement; and (2) bias in the ascertainment of ambulance dispatch causes. This review suggests that heat exposure is associated with an increased risk of ambulance dispatches, and there is a dose-response relationship between heatwave intensity and the risk of ambulance dispatches. For future studies assessing the heat-ambulance association, we recommend that (1) using data on spatially refined gridded temperature that is either very well interpolated or derived from satellite imaging may be an alternative to reduce exposure measurement bias; and (2) linking ambulance data with hospital admission data can be useful to improve health outcome classification.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
High ambient temperatures (i.e. heat) can adversely impact human health; including but not limited to the circulatory (Liu et al. 2022), respiratory (Cheng et al. 2019), renal (Liu et al. 2021a), nervous (Liu et al. 2021b), and endocrine systems (Moon 2021). Even in advanced economies, extreme heat is the most deadly natural hazard (Borden and Cutter 2008). Extreme heat, which already causes US $727 billion in economic losses worldwide each year (Callahan and Mankin 2022), is becoming more frequent and intense due to climate change.
Multi-national studies have reported an increased risk of mortality associated with heat (Guo et al. 2018; Vicedo-Cabrera et al. 2018). The effect of heat on healthcare services (e.g. hospital admissions) has previously been meta-analysed (Phung et al. 2016). Some recent studies have found that dispatch call centres and ambulances can more readily detect the acute effects of heat (Wang et al. 2021; Xu et al. 2018). Compared with emergency department presentation and hospital admission data, ambulance data allows for a more sensitive indication of total demand for health services allowing for better preparation, management, and deployment during heat events (Bassil 2010). It is worthwhile synthesising published evidence on heat and ambulance service use.
We systematically reviewed and summarised evidence provided in the available literature on heat, prolonged heat (i.e. heatwaves) and ambulance service use, aiming to (1) provide a pooled effect estimate for the impacts of heat and heatwaves on all-cause and cause-specific ambulance dispatches; and (2) identify potential sources of bias in the study methodology.
Materials and methods
This review was conducted in alignment with the most up-to-date version of Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Guidelines (Page et al. 2021), and a protocol was registered through the international prospective register of systematic reviews (PROSPERO Reference: CRD42022296556).
Eligibility criteria
Empirical studies were considered eligible for inclusion within the review if they met the following criteria: (1) human population; (2) English language; (3) published within the last decade (2011–2022); (4) included a measure of heat or heatwaves as the primary exposure; (5) used routinely collected ambulance records to investigate outcomes; (6) the outcome was public health-related (e.g. not performance assessment of ambulance services, nor occupational based). In this review, we defined heat as temperatures above an optimal temperature range or optimal temperature point which have adverse impacts on human health and well-being (Asseng et al. 2021; Gasparrini et al. 2015). As this review focused on the impact of short-term exposure to heat or heatwaves on the risk of ambulance dispatches, we included studies with the two most common designs which quantify the association between short-term exposure to heat or heatwaves and risk of health outcomes: time-series and case-crossover designs (Wu et al. 2022).
There were three exclusion criteria: (1) any studies relying exclusively on hospital, death registry, or emergency department admission records were excluded; (2) as the primary exposure of interest was heat and heatwaves, if any study investigated the impact of air pollution as the primary exposure, and included temperature as a confounding exposure, then these studies were also excluded. Temperature is a potential confounder of the association between short-term exposure to air pollution (particularly ozone) and the risk of health outcomes. For instance, the concentrations of ozone tend to increase during hot weather, and the association between short-term exposure to ozone and the risk of health outcomes may be confounded by heat (Alari et al. 2023). Air pollution has been found to be a modifier of the association between short-term heat exposure and the risk of health outcomes (Hu et al. 2022); (3) any study where the performance or evaluation of ambulance and emergency services occurred without evaluation of the public health impacts of heat again were excluded.
Information sources
After consultation with a research librarian at Griffith University, a search strategy was developed and applied to the following six online databases: PubMed, Embase, Cumulative Index of Nursing and Allied Health Literature (CINHAL), Scopus, ProQuest, and Web of Science. The search strategy consisted of three major themes: (i) a heat term, (ii) an ambulance term, and (iii) a health term. Terms were adjusted to each database using mesh terms and filters where applicable (Supplementary 1). Pilot searches were conducted to ensure search strategy robustness and inclusion of key literature, the final search was conducted on August 31, 2022. The references of identified articles were screened to make sure all relevant articles were included.
Literature selection and quality assessment
All study results acquired from the six databases searched were imported into Endnote (version X9, 2013), and duplicates were removed before being uploaded into Covidence (v2715, 2021) to complete data extraction and quality assessments. All study titles, abstracts, and full texts were screened by two independent reviewers (JW, and AB, SR, DP, or ZX) using standardised criteria. Any disagreements were resolved via discussion between both reviewers, and if consensus could not be reached, a third reviewer was introduced.
Quality assessment analyses were conducted by two reviewers (JW, and AB, SR, DP, or ZX) using the Newcastle-Ottawa Scale for assessing the quality of nonrandomised studies. The tool was adapted to suit each of the included study designs (time-series and case-crossover). Quality assessment analyses aided in assessing the quality of evidence presented within each study by examining sample representativeness, ascertainment of exposure and outcome measures, inclusion of common confounders within the statistical models used, and the specificity of the outcome presented (Supplementary 2).
Meta-analysis
For studies assessing the impact of heat on ambulance dispatches, if they used the same temperature indicator (e.g. mean temperature) and health outcome (e.g. ambulance dispatches for cardiovascular diseases), they were included in the same meta-analysis. The definitions of different temperature indicators used in the included studies are presented in the Supplementary 3. Twenty-three studies were excluded from the meta-analysis mainly due to the temperature indicators used:
Six studies used mean temperature as the temperature indicator (Cheng et al. 2016; Hu et al. 2020; Kotani et al. 2018; Onozuka and Hagihara 2015; Prichard et al. 2022; Wu et al. 2021). However, Cheng et al. used warm season temperature to examine the overall effect of heatwaves, Hu et al. used warm season temperature to examine the main and added effects of heatwaves, and Kotani et al., Onozuka and Hagihara, Prichard et al., and Wu et al. did not provide information on the specific values of the temperature cut-offs to define heat. Hence, the effect estimates published in these studies could not be pooled together.
Four studies used apparent temperature (Alessandrini et al. 2011; Hartz et al. 2013; Ng et al. 2014; Pourshaikhian et al. 2019). However, Alessandrini et al. used mean apparent temperature and dichotomised mean apparent temperature into “25 °C to 30 °C” and “> 30 °C”, Hartz et al. used maximum apparent temperature as the temperature indicator and heat-related illnesses as the health outcome, Ng et al. used maximum 3-h apparent temperature as the temperature indicator and heatstroke as the health outcome, and Pourshaikhian et al. used apparent temperature as the temperature indicator and cardiovascular diseases as the health outcomes.
Four studies used local heatwave definitions which were different from each other (Loughnan et al. 2014; Schaffer et al. 2012; Williams et al. 2011; Williams et al. 2020).
Three studies used maximum temperature (Romani et al. 2020; Turner et al. 2013; Williams et al. 2012). However, Romani et al. did not provide information on the values of the 95th percentile (i.e. heat definition) and used cardiovascular diseases as the health outcome, Turner et al. assessed the main and added effects of heatwaves on the risk of cause-specific ambulance dispatches, and Williams et al. assessed the association between maximum temperature and ambulance dispatches for all causes.
Two studies used heat index (Mathes et al. 2017; Zottarelli et al. 2021). However, Mathes et al. examined the association between heatwave and heat-related ambulance dispatches, and Zottarelli et al. assessed the association between heat and ambulance dispatches for all causes.
Two studies used excess heat factor (EHF) (Hatvani-Kovacs et al. 2016; Patel et al. 2019). However, the EHF definitions they used were different from each other, and they were different from the EHF definition used in the other two studies included in the meta-analysis (Jegasothy et al. 2017; Williams et al. 2018).
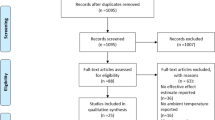
One study used humidex as the temperature indicator (Calkins et al. 2016). Fig. 1

The PRISMA diagram for literature selection flow
One study used compound heat as the temperature indicator (He et al. 2021).
Although there were studies using the same temperature indicator and out-of-hospital cardiac arrest (OHCA), we did not conduct a meta-analysis for OHCA because a separate meta-analysis has been published (Wu et al. 2023). We made two assumptions in the meta-analysis:
We assumed that odds ratio (OR) is a reasonable approximation of relative risk (RR) in the eligible studies because ambulance dispatches are small probability events (i.e. < 1%). Four eligible studies used RR as the effect estimate indicator (Cui et al. 2020; Sangkharat et al. 2020; Wang et al. 2021; Zhan et al. 2018), and Guo’s study used OR (Guo 2017). We assumed OR is a reasonable approximation of RR in Guo’s study. The study of Turner et al. used “percentage change in the risk of ambulance dispatches”, and we also converted it into RR.
We assumed that the association between heat and risk of ambulance dispatches is linear, acknowledging that the association between temperature (i.e. heat and cold) and health outcomes could be U-, J-, or V-shaped. Hence, we converted the RRs under different temperature increments reported in all six eligible studies (Cui et al. 2020; Guo 2017; Sangkharat et al. 2020; Turner et al. 2012; Wang et al. 2021; Zhan et al. 2018) into RRs per 5 °C increase in temperature. This approach has been used elsewhere (Chersich et al. 2020). The linear association between heat and risk of ambulance dispatches in the six eligible studies was shown in the figures of the six published papers (see Figure 2 of Cui et al. 2020, Figure 3 of Guo et al. 2017, Figure 3 of Sangkharat et al. 2020 (mainly for one ambulance dispatch indicator ‘999 ambulance’ but slightly different for the other indicator ‘Red ambulance’), Figure 2 of Wang et al. 2021, and Figure 2 of Zhan et al. 2018 (at lag 0)).

Forest plot for the association between heat and risk of ambulance dispatches

Forest plot for the association between heatwaves (defined by excess heat factor) and risk of ambulance dispatches
The impact of heat on ambulance dispatches may last for more than 1 day (i.e. lagged) but is generally acute. Cui et al. reported RRs across multiple lags (from lag 0–12 h to lag 0–170 h-) (Cui et al. 2020), and Sangkharat et al. reported RRs from 0–2 days to 0–21 days (Sangkharat et al. 2020). We used RRs for lags within 2 days in the meta-analysis because they generally represented the most acute impact of heat (Thomas et al. 2021; Winquist et al. 2016). The acute impact of heat occurred within 2 days was shown in the tables of the three published papers (see Table 2 of Cui et al. 2020, Table 3 of Sangkharat et al. 2020, and Table 3 of Turner et al. 2012).
For studies assessing the impact of heatwaves on ambulance dispatches, if they used the same heatwave definition (e.g. Excess Heat Factor (EHF)), effect estimate indicator (e.g. incidence rate ratio (IRR)), and health outcome (e.g. the daily total number of ambulance dispatches), they were included in the same meta-analysis. Specifically, two Australian studies which used EHF, in the same way, were pooled together (Jegasothy et al. 2017; Williams et al. 2018), and another two studies which used the same heatwave intensity (90th, 95th, or 99th percentiles) and duration indicators (2 or 3 days) were pooled together (Sun et al. 2014; Xu et al. 2018).
Random-effects models were used to pool the effect estimates. For studies which reported RRs across multiple lag periods within 2 days (e.g. 0–12, 0–24, and 0–48 h) (Cui et al. 2020), multiple regions (Williams et al. 2018), or multiple ambulance dispatch indicators (Sangkharat et al. 2020), we used hierarchical random-effects models to pool their RRs with RRs in other studies, accounting for both within-study variability (first level) and between-study variability (second level).
As the number of studies included in each meta-analysis was low (≤ 6), we were unable to assess a funnel plot or do more advanced regression-based assessments to evaluate publication bias.
Results
Study selection
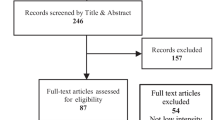
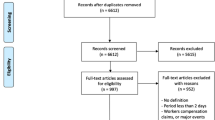
The PRISMA diagram in Fig. 1 describes the process of record selection for both the initial database searches and bibliographic screening. The final search yielded 3628 results from the six databases. Following title and abstract screening, this was reduced to 144 studies. After full-text and reference screenings, 48 full texts have been included in this review.
Quality assessments
Tables 1 and 2 display the quality assessment results for time-series (n = 42) and case-crossover studies (n = 6), respectively. Four of the included studies (n = 48) were of high quality, and the remaining 44 studies were of moderate quality. Among the four high-quality studies, three were of time-series design and one of case-crossover design.
Study characteristics
Table 3 displays the individual study characteristics and methodological parameters for all 48 studies. Among all the countries/regions, Australia had the highest number of included studies (n = 14) (Campbell et al. 2021; Doan et al. 2021; Guo 2017; Hatvani-Kovacs et al. 2016; Jegasothy et al. 2017; Loughnan et al. 2014; Patel et al. 2019; Schaffer et al. 2012; Turner et al. 2012, 2013; Williams et al. 2011; Williams et al. 2012; Williams et al. 2018; Xu et al. 2018), followed by mainland China (n = 11) (Cheng et al. 2016; Cui et al. 2020; He et al. 2021; Hu et al. 2020; Li et al. 2011; Niu et al. 2016; Sun et al. 2014; Wang et al. 2021; Wu et al. 2021; Yang et al. 2016; Zhan et al. 2018), Japan (n=6) (Fujitani et al. 2019; Kotani et al. 2018; Ng et al. 2014; Onozuka and Hagihara 2015, 2017; Takahashi and Shimadzu 2015), USA (n = 6) (Calkins et al. 2016; Hartz et al. 2013; Mathes et al. 2017; Williams et al. 2020; Zottarelli et al. 2021; DeVine et al. 2017), Taiwan (n = 2) (Lin et al. 2021; Wang et al. 2020), UK (n = 2) (Prichard et al. 2022; Sangkharat et al. 2020), Germany (n = 1) (Ghada et al. 2021), Iran (n = 1) (Pourshaikhian et al. 2019), Israel (n = 1) (Kranc et al. 2021), Italy (n = 1) (Alessandrini et al. 2011), Korea (n = 1) (Kim et al. 2012), Spain (n = 1) (Romani et al. 2020), and Sweden (n = 1) (Dahlquist et al. 2016).
Meta-analysis
Ten studies were eligible for meta-analysis (Table 3), with nine being of moderate quality. The only high-quality study was included in the meta-analysis on the association between heat and risk of ambulance dispatches for all causes (Sangkharat et al. 2020). For each 5 °C increase in mean temperature, the risk of ambulance dispatches for all causes and for cardiovascular diseases increased by 7% (95% confidence interval (CI): 5%, 10%) and 2% (95% CI: 1%, 3%), respectively (Fig. 2). The pooled statistics suggested that the risk of ambulance dispatches for respiratory diseases did not increase when the mean temperature increased.
For heatwaves defined by EHF, low-intensity, severe, and extreme heatwaves were associated with 6% (95% CI: 4%, 7%), 7% (95% CI: 5%, 9%), and 18% (95% CI: 12%, 23%) increases in the risk of ambulance dispatches, respectively (Fig. 3). For heatwaves defined by the incorporation of intensity and duration indicators, relatively mild (90th percentile) and very intense (99th percentile) heatwaves were associated with 2% and 3% increases in the risk of ambulance dispatches, respectively (Fig. 4).

Forest plot for the association between heatwaves (defined by threshold and intensity indicators) and risk of ambulance dispatches
Potential sources of bias in the included studies
We observed two potential sources of bias in the included studies: (1) bias in temperature exposure measurement; and (2) bias in ascertainment of ambulance dispatch causes.
A wide range of temperature indicators have been used in the included studies, including mean temperature, maximum temperature, minimum temperature, apparent temperature, humidex, and heat index. Mean temperature was the most commonly used temperature indicator (n = 28). Although spatially refined gridded data on temperature is increasingly accessible, 29 of the 48 studies only used temperature data collected from a single weather monitoring station for each study site (Table 3).
Half of the 48 studies included all-cause ambulance dispatches. A limited number of studies reported specific heat-related events (e.g. heatstroke, dehydration, heat exhaustion) (n = 6), cardiovascular (n = 17), and/or respiratory (n = 11) diseases. However, six studies on cause-specific ambulance dispatches did not publish or published less explicit information on how the ambulance dispatch causes were ascertained (Cui et al. 2020; Lin et al. 2021; Turner et al. 2012, 2013; Wang et al. 2021; Wang et al. 2020).
Discussion
Studies included in this review suggested a higher risk of ambulance dispatches associated with heat or heatwaves, although 44 of the 48 included studies were of moderate quality. The pooled statistics showed that each 5 °C increase in mean temperature was associated with 7% and 2% increases in the risks of ambulance dispatches for all causes and cardiovascular diseases, respectively. There appeared to be a dose-response relationship between EHF-defined heatwave intensity and the risk of ambulance dispatches.
Exposure to heat can trigger acute life-threatening cardiovascular diseases, such as acute myocardial infarction (Chen et al. 2019) and stroke (Bai et al. 2018). Heat exposure can also trigger acute kidney injury (Borg et al. 2017). The risk of ambulance dispatches increases when the risk of these acute diseases elevates during hot days at a population level. The dose-response relationship between EHF-defined heatwave intensity and the risk of ambulance dispatches, which we observed in the present review, echoed the findings in a recent Australian study which observed a dose-response relationship between heatwave intensity and mortality risk (Xu et al. 2023).
Although we purposely included studies using the two most ideal study designs in quantifying the association between short-term heat exposure and risk of health outcomes (i.e. time-series (Bhaskaran et al. 2013) and case-crossover (Carracedo-Martínez et al. 2010)), the quality of the included studies could have been better if two aspects of the methodology were improved: temperature exposure measurement and ascertainment of ambulance dispatch causes.
Temperature indicator and temperature exposure measurement
One of the main goals of conducting heat and health research is to facilitate health elements to be incorporated into the development and optimisation of heat adaptation strategies. Different temperature indicators have been used in different countries’ heat early warning systems (HEWS) (sometimes called heat-health action systems). For instance, Australia’s jurisdictional HEWS mainly use the excess heat factor to define heatwaves and trigger heat responses (e.g. the Queensland Heatwave Management Sub-plan (Queensland Health 2019)), and China’s national heatwave alert system uses maximum temperature as the temperature indicator for heatwave definition (China Meteorological Administration 2007). In heat and health research, using the temperature indicator that has been adopted in the national, regional, or local HEWS would facilitate the translation of research outputs into practice. For those countries/regions without HEWS, it is worthwhile conducting research to understand which temperature indicator performs better in predicting heat-related ambulance dispatches (Yu et al. 2011).
Heat exposure could vary within cities (e.g. urban heat island effect), and using temperature data collected from a single monitoring station may underestimate the impact of heat on morbidity if the monitoring station is less representative of heat-vulnerable populations’ exposure (Thomas et al. 2021). With the advent of publicly accessible and well-interpolated temperature data with high spatial resolution (e.g. the 5 km grided temperature data in Australia: https://www.longpaddock.qld.gov.au/silo/, or the worldwide ERA5-Land data at 9 km (Muñoz Sabater 2019) that can be further statistically downscaled to 900 m with KrigR (Byers et al. 2022)), it is possible to use these spatially refined gridded temperature data as an alternative to reduce potential measurement bias. However, we acknowledge that if the spatially refined temperature data was poorly interpolated, it could also cause bias. In the case where publicly accessible and well-interpolated temperature data with high spatial resolution is not available, satellite remote sensing temperature data could also be an option to reduce measurement bias (Xu et al. 2014) (e.g. satellite remote sensing data provided by the US National Aeronautics and Space Administration (NASA): https://ladsweb.modaps.eosdis.nasa.gov/). Because population density may vary across urban and rural areas within cities, Weinberger et al. have used population-weighted temperature derived from spatially refined gridded temperature data (Weinberger et al. 2019), attempting to reduce the temperature measurement bias. In the available studies comparing the health impacts of heat exposure using temperature data collected from limited number of monitoring stations and using spatially refined temperature data, because the models were fitted to the same health outcome and were non-nested, they were unable to quantify the magnitude of the temperature measurement bias. Simulation studies, such as what Wei et al. did in air pollution epidemiology (Wei et al. 2022), will help characterise the magnitude of temperature measurement bias.
Causes of ambulance dispatches
A main barrier to understanding the potential causal relationship between exposure to heat or heatwaves and the risk of ambulance dispatches is the lack of cause-specific ambulance dispatch data. Some studies included in the present review reported cause-specific ambulance dispatch data. For instance, Campbell et al. used data on ambulance dispatches for cardiovascular, respiratory, renal, diabetic, psychological, direct heat-related, and other heat-related conditions in Tasmania, Australia (Campbell 2021), and they clarified that the records on causes were completed by attending paramedics at the time of, or right after the incident requiring ambulance dispatches.
Unless the patients who used ambulance service have later been hospitalised and gone through diagnostic examinations, it may be hard to accurately ascertain the true causes of ambulance dispatches (particularly in elderly patients who often have multimorbidity (Dobson et al. 2020)). In the present review, the pooled statistics did not suggest an association between heat and the risk of ambulance dispatches for respiratory diseases, but we could not rule out the possibility that respiratory diseases might not have been properly ascertained in the included studies. Data linkage could be an alternative to solve this conundrum. For instance, the information on ICD-codes (international classification of diseases) is generally available in emergency department visit or hospitalisation data. Therefore, linking patients’ ambulance dispatch data with their emergency department visit or hospitalisation data could allow researchers to obtain more accurate information on the causes of ambulance dispatches (Vallmuur et al. 2023).
Conclusion
The available epidemiological evidence suggests that each 5 °C increase in mean temperature is associated with 7% and 2% increases in the risks of all-cause and cardiovascular ambulance dispatches, respectively. There is a dose-response relationship between EHF-defined heatwave intensity and the risk of all-cause ambulance dispatches. Future studies using well-interpolated or satellite-derived data on spatially refined gridded temperature and linking ambulance data with hospital data may be useful in reducing biases in exposure measurement and health outcome classification.
References
Alari A, Chen C, Schwarz L, Hdansen K, Chaix B, Benmarhnia T (2023) The role of ozone as a mediator of the eelationship between heat waves and mortality in 15 French urban areas. Am J Epidemiol. https://doi.org/10.1093/aje/kwad032
Alessandrini E, Zauli Sajani S, Scotto F, Miglio R, Marchesi S, Lauriola P (2011) Emergency ambulance dispatches and apparent temperature: a time series analysis in Emilia-Romagna Italy. Environ Res 111(8):1192–1200. https://doi.org/10.1016/j.envres.2011.07.005
Asseng S, Spänkuch D, Hernandez-Ochoa IM, Laporta J (2021) The upper temperature thresholds of life. Lancet Planet Health 5(6):e378–e385. https://doi.org/10.1016/S2542-5196(21)00079-6
Bai L, Li Q, Wang J, Lavigne E, Gasparrini A, Copes R, Yagouti A, Burnett RT, Goldberg MS, Cakmak S, Chen H (2018) Increased coronary heart disease and stroke hospitalisations from ambient temperatures in Ontario. Heart 104(8):673–679. https://doi.org/10.1136/heartjnl-2017-311821
Bassil K (2010) Surveillance of heat-related illness with ambulance dispatch data. VDM Verlag
Bhaskaran K, Gasparrini A, Hajat S, Smeeth L, Armstrong B (2013) Time series regression studies in environmental epidemiology. Int J Epidemiol 42(4):1187–1195. https://doi.org/10.1093/ije/dyt092
Borden KA, Cutter SL (2008) Spatial patterns of natural hazards mortality in the United States. Int J Health Geogr 7:64. https://doi.org/10.1186/1476-072x-7-64
Borg M, Bi P, Nitschke M, Williams S, McDonald S (2017) The impact of daily temperature on renal disease incidence: an ecological study. Environ Health 16(1):114. https://doi.org/10.1186/s12940-017-0331-4
Byers J, Bao L, Carson J, Gill J (2022) Krige: geospatial kriging with metropolis sampling. Available from: https://CRAN.R-project.org/package=krige.
Calkins MM, Isaksen TB, Stubbs BA, Yost MG, Fenske RA (2016) Impacts of extreme heat on emergency medical service calls in King County, Washington, 2007-2012: relative risk and time series analyses of basic and advanced life support. Environ Health 15:13. https://doi.org/10.1186/s12940-016-0109-0
Callahan CW, Mankin JS (2022) Globally unequal effect of extreme heat on economic growth. Sci Adv 8. https://doi.org/10.1126/sciadv.add3726
Campbell SL, Remenyi T, Williamson GJ, Rollins D, White CJ, Johnston FH (2021) Ambulance dispatches and heatwaves in Tasmania, Australia: a case-crossover analysis. Environ Res 202:111655. https://doi.org/10.1016/j.envres.2021.111655
Carracedo-Martínez E, Taracido M, Tobias A, Saez M, Figueiras A (2010) Case-crossover analysis of air pollution health effects: a systematic review of methodology and application. Environ Health Perspect 118(8):1173–1182. https://doi.org/10.1289/ehp.0901485
Chen K, Breitner S, Wolf K, Hampel R, Meisinger C, Heier M, von Scheidt W, Kuch B, Peters A, Schneider A (2019) Temporal variations in the triggering of myocardial infarction by air temperature in Augsburg, Germany, 1987-2014. Eur Heart J 40(20):1600–1608. https://doi.org/10.1093/eurheartj/ehz116
Cheng J, Xu Z, Zhao D, Xie M, Zhang H, Wang S, Su H (2016) The burden of extreme heat and heatwave on emergency ambulance dispatches: a time-series study in Huainan, China. Sci Total Environ 571:27–33. https://doi.org/10.1016/j.scitotenv.2016.07.103
Cheng J, Xu Z, Bambrick H, Prescott V, Wang N, Zhang Y, Su H, Tong S, Hu W (2019) Cardiorespiratory effects of heatwaves: a systematic review and meta-analysis of global epidemiological evidence. Environ Res 177:108610. https://doi.org/10.1016/j.envres.2019.108610
Chersich MF, Pham MD, Areal A, Haghighi MM, Manyuchi A, Swift CP, Wernecke B, Robinson M, Hetem R, Boeckmann M, Hajat S (2020) Associations between high temperatures in pregnancy and risk of preterm birth, low birth weight, and stillbirths: systematic review and meta-analysis. BMJ 371:m3811. https://doi.org/10.1136/bmj.m3811
China Meteorological Administration (2007). Heat warning signals. https://www.cma.gov.cn/kppd/kppdqxwq/kppdfzbd/201212/t20121217_197852.html. Accessed 19 January 2023.
Cui Y, Ai S, Liu Y, Qian ZM, Wang C, Sun J, Sun X, Zhang S, Syberg KM, Howard S, Qin L, Lin H (2020) Hourly associations between ambient temperature and emergency ambulance calls in one central Chinese city: call for an immediate emergency plan. Sci Total Environ 711:135046. https://doi.org/10.1016/j.scitotenv.2019.135046
Dahlquist M, Raza A, Bero-Bedada G, Hollenberg J, Lind T, Orsini N, Sjögren B, Svensson L, Ljungman PL (2016) Short-term departures from an optimum ambient temperature are associated with increased risk of out-of-hospital cardiac arrest. Int J Hyg Environ Health 219(4-5):389–397. https://doi.org/10.1016/j.ijheh.2016.03.005
DeVine AC, Vu PT, Yost MG, Seto EYW, Busch Isaksen TM (2017) A geographical analysis of emergency medical service calls and extreme heat in King County, WA, USA (2007-2012). Int J Environ Res Public Health 14(8). https://doi.org/10.3390/ijerph14080937
Doan TN, Wilson D, Rashford S, Bosley E (2021) Ambient temperatures, heatwaves and out-of-hospital cardiac arrest in Brisbane, Australia. Occup Environ Med. https://doi.org/10.1136/oemed-2020-107018
Dobson A, Forder P, Hockey R, Egan N, Cavenagh D, Waller M, Xu Z, Anderson A, Byrnes E, Barnes I, Loxton D, Byles J, Mishra G (2020) The impact of chronic conditions: findings from the Australian Longitudinal Study on Women’s Health. Report prepared for the Australian Government Department of Health
Fujitani Y, Otani S, Majbauddin A, Amano H, Masumoto T, Kurozawa Y (2019) Impact of maximum air temperature on ambulance transports owing to heat stroke during spring and summer in Tottori Prefecture, Japan: a time-stratified case-crossover analysis. Yonago Acta Med 62(1):47–52. https://doi.org/10.33160/yam.2019.03.007
Gasparrini A, Guo Y, Hashizume M, Lavigne E, Zanobetti A, Schwartz J, Tobias A, Tong S, Rocklöv J, Forsberg B, Leone M, De Sario M, Bell ML, Guo Y-LL, Wu C-f, Kan H, Yi S-M, PHN S, Honda Y et al (2015) Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet 386(9991):369–375. https://doi.org/10.1016/S0140-6736(14)62114-0
Ghada W, Estrella N, Pfoerringer D, Kanz KG, Bogner-Flatz V, Ankerst DP, Menzel A (2021) Effects of weather, air pollution and Oktoberfest on ambulance-transported emergency department admissions in Munich. Germany Sci Total Environ 755(Pt 2):143772. https://doi.org/10.1016/j.scitotenv.2020.143772
Guo Y (2017) Hourly associations between heat and ambulance calls. Environ Pollut 220(Pt B):1424–1428. https://doi.org/10.1016/j.envpol.2016.10.091
Guo Y, Gasparrini A, Li S, Sera F, Vicedo-Cabrera AM et al (2018) Quantifying excess deaths related to heatwaves under climate change scenarios: a multicountry time series modelling study. PLoS Med 15(7):e1002629. https://doi.org/10.1371/journal.pmed.1002629
Hartz DA, Brazel AJ, Golden JS (2013) A comparative climate analysis of heat-related emergency 911 dispatches: Chicago, Illinois and Phoenix, Arizona USA 2003 to 2006. Int J Biometeorol 57(5):669–678. https://doi.org/10.1007/s00484-012-0593-z
Hatvani-Kovacs G, Belusko M, Pockett J, Boland J (2016) Can the excess heat factor indicate heatwave-related morbidity? A case study in Adelaide. South Australia Ecohealth 13(1):100–110. https://doi.org/10.1007/s10393-015-1085-5
He Y-L, Deng S-Z, Ho HC, Wang H-B, Chen Y, Hajat S, Ren C, Zhou B-Q, Cheng J, Hu W, Ma W-J, Huang C-R (2021) The half-degree matters for heat-related health impacts under the 1.5 °C and 2 °C warming scenarios: evidence from ambulance data in Shenzhen, China. Adv Clim Chang Res 12(5):628–637. https://doi.org/10.1016/j.accre.2021.09.001
Hu J, Wen Y, Duan Y, Yan S, Liao Y, Pan H, Zhu J, Yin P, Cheng J, Jiang H (2020) The impact of extreme heat and heat waves on emergency ambulance dispatches due to external cause in Shenzhen. China Environ Pollut 261:114156. https://doi.org/10.1016/j.envpol.2020.114156
Hu X, Han W, Wang Y, Aunan K, Pan X, Huang J, Li G (2022) Does air pollution modify temperature-related mortality? A systematic review and meta-analysis. Environ Res 210:112898. https://doi.org/10.1016/j.envres.2022.112898
Jegasothy E, McGuire R, Nairn J, Fawcett R, Scalley B (2017) Extreme climatic conditions and health service utilisation across rural and metropolitan New South Wales. Int J Biometeorol 61(8):1359–1370. https://doi.org/10.1007/s00484-017-1313-5
Kim Y, Kim H, Shin SD, Hong YC (2012) Different influence of outdoor temperature on traumatic and nontraumatic injuries. J Trauma Acute Care Surg 73(4):944–949. https://doi.org/10.1097/TA.0b013e318256de02
Kotani K, Ueda K, Seposo X, Yasukochi S, Matsumoto H, Ono M, Honda A, Takano H (2018) Effects of high ambient temperature on ambulance dispatches in different age groups in Fukuoka. Japan Glob Health Action 11(1):1437882. https://doi.org/10.1080/16549716.2018.1437882
Kranc H, Novack V, Shtein A, Sherman R, Novack L (2021) Extreme temperature and out-of-hospital-cardiac-arrest. Nationwide study in a hot climate country. Environ Health 20(1):38. https://doi.org/10.1186/s12940-021-00722-1
Li Y, Du T, Lewin MR, Wang H, Ji X, Zhang Y, Xu T, Xu L, Wu JS (2011) The seasonality of acute coronary syndrome and its relations with climatic parameters. Am J Emerg Med 29(7):768–774. https://doi.org/10.1016/j.ajem.2010.02.027
Lin YK, Cheng CP, Kim H, Wang YC (2021) Risk of ambulance services associated with ambient temperature, fine particulate and its constituents. Sci Rep 11(1):1651. https://doi.org/10.1038/s41598-021-81197-5
Liu J, Varghese BM, Hansen A, Borg MA, Zhang Y, Driscoll T, Morgan G, Dear K, Gourley M, Capon A, Bi P (2021a) Hot weather as a risk factor for kidney disease outcomes: a systematic review and meta-analysis of epidemiological evidence. Sci Total Environ 801:149806. https://doi.org/10.1016/j.scitotenv.2021.149806
Liu J, Varghese BM, Hansen A, Xiang J, Zhang Y, Dear K, Gourley M, Driscoll T, Morgan G, Capon A, Bi P (2021b) Is there an association between hot weather and poor mental health outcomes? A systematic review and meta-analysis. Environ Int 153:106533. https://doi.org/10.1016/j.envint.2021.106533
Liu J, Varghese BM, Hansen A, Zhang Y, Driscoll T, Morgan G, Dear K, Gourley M, Capon A, Bi P (2022) Heat exposure and cardiovascular health outcomes: a systematic review and meta-analysis. Lancet Planet Health 6(6):e484–e495. https://doi.org/10.1016/s2542-5196(22)00117-6
Loughnan ME, Tapper NJ, Phan T, McInnes JA (2014) Can a spatial index of heat-related vulnerability predict emergency service demand in Australian capital cities? Int J Emerg 3(1):6–33
Mathes RW, Ito K, Lane K, Matte TD (2017) Real-time surveillance of heat-related morbidity: Relation to excess mortality associated with extreme heat. PLoS One 12(9):e0184364. https://doi.org/10.1371/journal.pone.0184364
Moon J (2021) The effect of the heatwave on the morbidity and mortality of diabetes patients; a meta-analysis for the era of the climate crisis. Environ Res 195:110762. https://doi.org/10.1016/j.envres.2021.110762
Muñoz-Sabater J, Dutra E, Agustí-Panareda A et al (2021) ERA5-Land: a state-of-the-art global reanalysis dataset for land applications. Earth Syst Sci Data 13(9):4349–4383. https://doi.org/10.5194/essd13-4349-2021
Ng CF, Ueda K, Ono M, Nitta H, Takami A (2014) Characterizing the effect of summer temperature on heatstroke-related emergency ambulance dispatches in the Kanto area of Japan. Int J Biometeorol 58(5):941–948. https://doi.org/10.1007/s00484-013-0677-4
Niu Y, Chen R, Liu C, Ran P, Chen A, Chen X, Kan H (2016) The association between ambient temperature and out-of-hospital cardiac arrest in Guangzhou, China. Sci Total Environ 572:114–118. https://doi.org/10.1016/j.scitotenv.2016.07.205
Onozuka D, Hagihara A (2015) All-cause and cause-specific risk of emergency transport attributable to temperature: a nationwide study. Medicine (Baltimore) 94(51):e2259. https://doi.org/10.1097/md.0000000000002259
Onozuka D, Hagihara A (2017) Extreme temperature and out-of-hospital cardiac arrest in Japan: a nationwide, retrospective, observational study. Sci Total Environ 575:258–264. https://doi.org/10.1016/j.scitotenv.2016.10.045
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Patel D, Jian L, Xiao J, Jansz J, Yun G, Robertson A (2019) Joint effect of heatwaves and air quality on emergency department attendances for vulnerable population in Perth, Western Australia, 2006 to 2015. Environ Res 174:80–87. https://doi.org/10.1016/j.envres.2019.04.013
Phung D, Thai PK, Guo Y, Morawska L, Rutherford S, Chu C (2016) Ambient temperature and risk of cardiovascular hospitalization: an updated systematic review and meta-analysis. Sci Total Environ 550:1084–1102. https://doi.org/10.1016/j.scitotenv.2016.01.154
Pourshaikhian M, Moghadamnia MT, Yekaninejad MS, Ghanbari A, Rashti AS, Afraz Kamachli S (2019) The effects of meteorological variables on ambulance attendance for cardiovascular diseases in Rasht. Iran J Therm Biol 83:150–156. https://doi.org/10.1016/j.jtherbio.2019.05.002
Prichard GC, Sangkharat K, Fisher PA, Thornes JE, Phalkey R, Pope FD (2022) Differential health responses to climate change projections in three UK cities as measured by ambulance dispatch data. Environ Adv 7:100146. https://doi.org/10.1016/j.envadv.2021.100146
Queensland Health (2019) Queensland heatwave management sub-plan. Report published by the State of Government. Available from: https://www.health.qld.gov.au/__data/assets/pdf_file/0032/628268/heatwaveresponse-plan.pdf
Romani SG, Royé D, Sánchez Santos L, Figueiras A (2020) Impact of extreme temperatures on ambulance dispatches due to cardiovascular causes in North-West Spain. Int J Environ Res Public Health 17(23). https://doi.org/10.3390/ijerph17239001
Sangkharat K, Mahmood MA, Thornes JE, Fisher PA, Pope FD (2020) Impact of extreme temperatures on ambulance dispatches in London. UK Environ Res 182:109100. https://doi.org/10.1016/j.envres.2019.109100
Schaffer A, Muscatello D, Broome R, Corbett S, Smith W (2012) Emergency department visits, ambulance calls, and mortality associated with an exceptional heat wave in Sydney, Australia, 2011: a time-series analysis. Environ Health 11(1):3. https://doi.org/10.1186/1476-069x-11-3
Sun X, Sun Q, Yang M, Zhou X, Li X, Yu A, Geng F, Guo Y (2014) Effects of temperature and heat waves on emergency department visits and emergency ambulance dispatches in Pudong New Area, China: a time series analysis. Environ Health 13:76. https://doi.org/10.1186/1476-069x-13-76
Takahashi K, Shimadzu H (2015) The daily incidence of out-of-hospital cardiac arrest unexpectedly increases around New Year’s Day in Japan. Resuscitation 96:156–162. https://doi.org/10.1016/j.resuscitation.2015.08.003
Thomas N, Ebelt ST, Newman AJ, Scovronick N, D’Souza RR, Moss SE, Warren JL, Strickland MJ, Darrow LA, Chang HH (2021) Time-series analysis of daily ambient temperature and emergency department visits in five US cities with a comparison of exposure metrics derived from 1-km meteorology products. Environ Health 20(1):55. https://doi.org/10.1186/s12940-021-00735-w
Turner LR, Connell D, Tong S (2012) Exposure to hot and cold temperatures and ambulance attendances in Brisbane, Australia: a time-series study. BMJ Open 2(4). https://doi.org/10.1136/bmjopen-2012-001074
Turner LR, Connell D, Tong S (2013) The effect of heat waves on ambulance attendances in Brisbane. Australia Prehosp Disaster Med 28(5):482–487. https://doi.org/10.1017/s1049023x13008789
Vallmuur K, McCreanor V, Watson A, Cameron C, Cramb S, Dias S, Banu S, Warren J (2023) Understanding compensable and non-compensable patient profiles, pathways and physical outcomes for transport and work-related injuries in Queensland. Australia through data linkage BMJ Open 13(1):e065608. https://doi.org/10.1136/bmjopen-2022-065608
Vicedo-Cabrera AM, Guo Y, Sera F, Huber V, Schleussner CF, Mitchell D, Tong S et al (2018) Temperature-related mortality impacts under and beyond Paris Agreement climate change scenarios. Clim Chang 150(3-4):391–402. https://doi.org/10.1007/s10584-018-2274-3
Wang YC, Lin YK, Chen YJ, Hung SC, Zafirah Y, Sung FC (2020) Ambulance services associated with extreme temperatures and fine particles in a subtropical island. Sci Rep 10(1):2855. https://doi.org/10.1038/s41598-020-59294-8
Wang Q, He Y, Hajat S, Cheng J, Xu Z, Hu W, Ma W, Huang C (2021) Temperature-sensitive morbidity indicator: consequence from the increased ambulance dispatches associated with heat and cold exposure. Int J Biometeorol 65(11):1871–1880. https://doi.org/10.1007/s00484-021-02143-8
Wei YA-O, Qiu X, Yazdi MA-O, Shtein A, Yang J, Shi LA-O, Peralta AA-OX, Coull BA, Schwartz J (2022) he impact of exposure measurement error on the estimated concentration-response relationship between long-term exposure to PM2.5 and mortality. Environ Health Perspect 130(7):77006
Weinberger KR, Spangler KR, Zanobetti A, Schwartz JD, Wellenius GA (2019) Comparison of temperature-mortality associations estimated with different exposure metrics. Environ Epidemiol 3(5):e072. https://doi.org/10.1097/ee9.0000000000000072
Williams S, Nitschke M, Tucker G, Bi P (2011) Extreme heat arrangements in South Australia: an assessment of trigger temperatures. Health Promot J Austr (22):S21–S27. https://doi.org/10.1071/he11421
Williams S, Nitschke M, Sullivan T, Tucker GR, Weinstein P, Pisaniello DL, Parton KA, Bi P (2012) Heat and health in Adelaide, South Australia: assessment of heat thresholds and temperature relationships. Sci Total Environ 414:126–133. https://doi.org/10.1016/j.scitotenv.2011.11.038
Williams S, Venugopal K, Nitschke M, Nairn J, Fawcett R, Beattie C, Wynwood G, Bi P (2018) Regional morbidity and mortality during heatwaves in South Australia. Int J Biometeorol 62(10):1911–1926. https://doi.org/10.1007/s00484-018-1593-4
Williams AA, Allen JG, Catalano PJ, Buonocore JJ, Spengler JD (2020) The influence of heat on daily police, medical, and fire dispatches in Boston, Massachusetts: relative risk and time-series analyses. Am J Public Health 110(5):662–668. https://doi.org/10.2105/ajph.2019.305563
Winquist A, Grundstein A, Chang HH, Hess J, Sarnat SE (2016) Warm season temperatures and emergency department visits in Atlanta, Georgia. Environ Res 147:314–323. https://doi.org/10.1016/j.envres.2016.02.022
Wu W, Chen B, Wu G, Wan Y, Zhou Q, Zhang H, Zhang J (2021) Increased susceptibility to temperature variation for non-accidental emergency ambulance dispatches in Shenzhen. China Environ Sci Pollut Res Int 28(24):32046–32056. https://doi.org/10.1007/s11356-021-12942-6
Wu K, Ho HC, Su H, Huang C, Zheng H, Zhang W, Tao J, Hossain MZ, Zhang Y, Hu K, Yang M, Wu Q, Xu Z, Cheng J (2022) A systematic review and meta-analysis of intraday effects of ambient air pollution and temperature on cardiorespiratory morbidities: first few hours of exposure matters to life. eBioMedicine 86:104327. https://doi.org/10.1016/j.ebiom.2022.104327
Wu Q, Yang M, Wu K, Su H, Huang C, Xu Z, Ho HC, Zheng H, Zhang W, Tao J, Dang TAT, Hossain MZ, Khan MA, Bogale D, Cheng J (2023) Abnormal ambient temperature change increases the risk of out-of-hospital cardiac arrest: a systematic review and meta-analysis of exposure types, risk, and vulnerable populations. Sci Total Environ 861:160554. https://doi.org/10.1016/j.scitotenv.2022.160554
Xu Z, Liu Y, Ma Z, Li S, Hu W, Tong S (2014) Impact of temperature on childhood pneumonia estimated from satellite remote sensing. Environ Res 132:334–341. https://doi.org/10.1016/j.envres.2014.04.021
Xu Z, Cheng J, Hu W, Tong S (2018) Heatwave and health events: a systematic evaluation of different temperature indicators, heatwave intensities and durations. Sci Total Environ 630:679–689. https://doi.org/10.1016/j.scitotenv.2018.02.268
Xu Z, Varghese BM, Trancoso R, Wilson LF, Cheng J, Tong S (2023) Mortality associated with heatwave severity in the three largest Australian cities. Epidemiology 34(1):e3–e4. https://doi.org/10.1097/ede.0000000000001551
Yang C, Chen X, Chen R, Cai J, Meng X, Wan Y, Kan H (2016) Daily ambient temperature and renal colic incidence in Guangzhou, China: a time-series analysis. Int J Biometeorol 60(8):1135–1142. https://doi.org/10.1007/s00484-015-1106-7
Yu W, Guo Y, Ye X, Wang X, Huang C, Pan X, Tong S (2011) The effect of various temperature indicators on different mortality categories in a subtropical city of Brisbane. Australia Sci Total Environ 409(18):3431–3437. https://doi.org/10.1016/j.scitotenv.2011.05.027
Zhan ZY, Yu YM, Qian J, Song YF, Chen PY, Ou CQ (2018) Effects of ambient temperature on ambulance emergency call-outs in the subtropical city of Shenzhen. China PLoS One 13(11):e0207187. https://doi.org/10.1371/journal.pone.0207187
Zottarelli LK, Sharif HO, Xu X, Sunil TS (2021) Effects of social vulnerability and heat index on emergency medical service incidents in San Antonio, Texas, in 2018. J Epidemiol Community Health 75(3):271–276. https://doi.org/10.1136/jech-2019-213256
Acknowledgements
We would like to thank Griffith University Climate Action Beacon and Wellcome. We are grateful to Professor Jian Cheng and Miss Qiyue Wu for their assistance in making the forest plots.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions This work was supported by Griffith University Climate Action Beacon seed funding and by Wellcome (224709/Z/21/Z: ‘Individualised heat-health early warning systems: A novel digital solution’).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Supplementary information
ESM 1
(DOCX 28 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xu, Z., Watzek, J.T., Phung, D. et al. Heat, heatwaves, and ambulance service use: a systematic review and meta-analysis of epidemiological evidence. Int J Biometeorol 67, 1523–1542 (2023). https://doi.org/10.1007/s00484-023-02525-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-023-02525-0